This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
She was brought in by ambulance and received aspirin and nitroglycerin en route. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Detailed coronary artery evaluation not performed.
The ambulance report says "BP continued to drop during transport and pt remained cold and clammy." Frick — an all-too-common misconception is that the absence of obstructive coronary disease on cardiac catheterization rules out acute coronary occlusion as the cause of the patient's acute event. This is not the case.
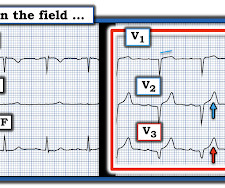
A 40-something male presented by ambulance with one hour of chest pain that was improving after sublingual nitroglycerine and 325 mg of aspirin, chewed. Or had not had a prehospital ECG on the ambulance. Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.) have perfect coronary flow by the time of angiogram.
The nitro she took in the ambulance did not help. If she had no risk factors, it is doubtful that she would have developed such extensive coronary artery disease as we see on the angiogram. Her first EKG in isolation has no hard findings that are diagnostic for an acute coronary occlusion.
I am sure that I posted it, but don't know when or where: This patient arrived to the ED by ambulance with chest pain that had resolved. Reference: • Writing Committee, Kontos MC, de Lemos JA, et al. Is the ability to diagnose posterior reperfusion a useful skill? Here is a case from a while back. They did, but had not recognized it.
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. Evaluation of T-wave morphology in patients with left bundle branch block and suspected acute coronary syndrome. 3] Meyers, H. 4] Dodd, K.
Paper: Van de Werf, F et al. STREAM-2: Half-Dose Tenecteplase or Primary Percutaneous Coronary Intervention in Older Patients With ST-Segment-Elevation Myocardial Infarction: A Randomized, Open-Label Trial. References: Van de Werf, F et al. PMID: 37439219 Armstrong P et al. Primary PCI: 95.7% Primary PCI: 95.7%
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. In fact, Kosuge et al. Stein et al. This is a paper worth reading : Marchik et al. Kosuge et al.
Background: Historically, we have treated acute coronary syndrome with supplemental oxygen regardless of the patient ’ s oxygen saturation. More recent evidence, however, demonstrates that too much oxygen could be harmful ( AVOID Trial ) by causing coronary vasoconstriction and increasing oxidative stress. Low O2 protocol: 3.1%
They did not have an ultrasound on the ambulance (some local crews are starting to utilize POC limited US in our service areas). See this paper by Smith et al. This is particularly true of RV MI: LV coronary perfusion is dependent on diastolic pressure because the myocardial pressure is too high for perfusion during systole.
This page summarises the most current recommendations for the management of acute coronary syndromes with persistent ST-segment elevations (i.e I B Ambulance personnel must be trained and equipped to identify STEMI and administer fibrinolysis if necessary. STEMI , ST-segment elevation acute myocardial infarction ).
Some of the critical differentials include pulmonary embolism, acute decompensated heart failure, pneumonia, pneumothorax, and acute coronary syndrome. Anginal chest pain, chest heaviness, or evidence of fluid overload suggest acute coronary syndrome or acute decompensated heart failure. Adeloye D, Song P, Zhu Y, et al.
The patient contacted the ambulance service after he experienced sudden onset chest pain and diaphoresis that had started 20 minutes prior. al in 2008, and is eponymously named after the main author. This typically occurs in the setting of a rapidly reperfused coronary artery following a myocardial infarction.
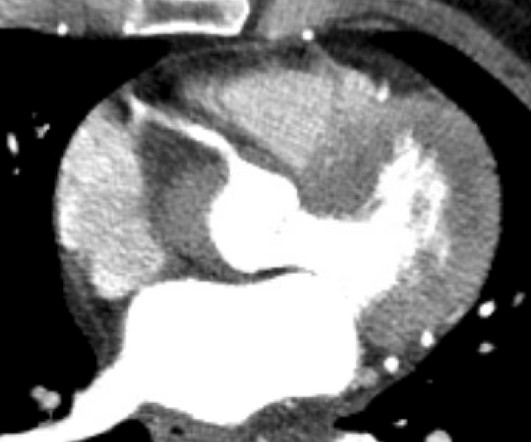
Cardiology wanted a CT of the aorta to rule out dissection, presumably partly due to the very high blood pressure readings, but also because it is hard for people to believe that a 20-something woman could have acute thrombotic coronary artery. Coronary malperfusion due to type A aortic dissection: mechanism and surgical management.
Initial 4th generation troponin I was 10 ng/mL is consistent with large MI due to acute coronary occlusion (OMI). It was in his central and left chest, radiated to his left arm, and he experienced some cold sweats and nausea prompting him to call 911 and he was brought to ED via ambulance. Lupu et al. Pain was decreased to 2/10.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content