This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background: Primary PCI is the recommended reperfusion strategy in patients with STEMI and should be initiated within 2 hours after first medical contact. Paper: Van de Werf, F et al. In non-PCI-capable hospitals this goal is not always achievable due to delays in transfer. Primary PCI: 95.7% Primary PCI: 95.7% Primary PCI: 78.4%
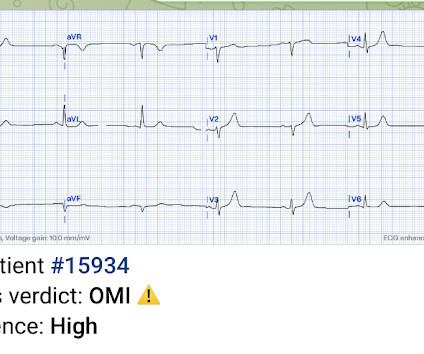
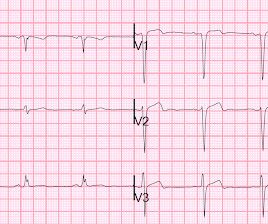
A 61 year-old with chest pain arrived to the ED by ambulance with resolving chest pain. link] Hughes KE et al. However, when I saw this patient, I knew that he had come by ambulance, so I knew there must be a prehospital ECG recorded somewhere and went to look for it. This ECG is NOT normal. There is low QRS amplitude.
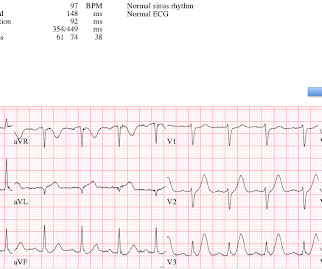
A 40-something male presented by ambulance with one hour of chest pain that was improving after sublingual nitroglycerine and 325 mg of aspirin, chewed. Here it is: Obvious Inferior Posterior STEMI (+) OMI. Or had not had a prehospital ECG on the ambulance. Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.)
She was brought in by ambulance and received aspirin and nitroglycerin en route. Lindahl et al. From Gue at al. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. In fact, Kosuge et al. Stein et al. This is a paper worth reading : Marchik et al. Kosuge et al.
Based on recent studies, current guidelines recommend that O2 should not be given to non-hypoxemic patients with STEMI or NSTEMI [2,3]. Click here for Direct Download of the Podcast Paper: Stewart, RAH et al. 4159 patients (10% of total population) had STEMI 30d Mortality: High O2 protocol: 8.8% PMID: 25260718 Ibanez B et al.
Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4. Finally, Transient STEMI should be taken emergently to the cath lab. Normalization of Diagnostic For STEMI Prehospital ECG with Nitroglycerin Therapy. If the initial ECG was diagnostic for STEMI the paramedic called to mobilize the reperfusion team.
STEMI , ST-segment elevation acute myocardial infarction ). 1 Initial diagnosis of STEMI ECG Management Recommendation Level of evidence A 12-lead ECG should be interpreted immediately (within 10 minutes) at first medical contact. I B Designated PCI centres should provide angiography and reperfusion 24/7 without delay.
link] In this paper, in a department in which they state they have only 50 STEMI per year, they looked at only 8 days worth of triage ECGs for a total of 538. They did not find one STEMI on their triage ECGs (no surprise! We at HCMC have 30 walk-in STEMIs per year; the rest come by ambulance. October 2018. Fair enough.
The ambulance report says "BP continued to drop during transport and pt remained cold and clammy." Figure-2: Classification of Underlying Diagnoses in Patients with MINOCA ( Adapted from Table-1 in Sykes et al: Interventional Cardiology Review: 16:e10, 2021 ).
You may have mastered all the latest changes affecting management of sepsis, STEMI, and opiate-use disorder, but there’s no stopping the relentless revisions to our approach to neurologic emergencies. It should sound familiar from its use in the early days for STEMI. References Li G, Lin Y, Yang J, et al. N Engl J Med.
There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI). In fact, the STE is widespread, mimicking an anterior STEMI. See this paper by Smith et al.
If it was a shockable rhythm, and the ECG is showing clear-cut STEMI, we want to activate the cardiac cath lab. In my system, we announce CODE-STEMI over the radio and get a time stamp, and we follow up with ECG transmission. References Callaway C, Donnino M, Fink E et al. All of your practice has just paid off. Circulation.
Here is the repeat ECG at 52 minutes after arrival to triage: Obvious posterolateral STEMI Angiographic findings: 1. I am sure that I posted it, but don't know when or where: This patient arrived to the ED by ambulance with chest pain that had resolved. Reference: • Writing Committee, Kontos MC, de Lemos JA, et al.
The nitro she took in the ambulance did not help. Patients like her are the reason we are advocating for a change in the ACS paradigm from STEMI to OMI. Armstrong et al attempted to study it but may have included too many 'obvious' cases - the criteria from that paper would certainly have missed this case.
The patient contacted the ambulance service after he experienced sudden onset chest pain and diaphoresis that had started 20 minutes prior. al in 2008, and is eponymously named after the main author. This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. How will you manage this patient?
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". It was in his central and left chest, radiated to his left arm, and he experienced some cold sweats and nausea prompting him to call 911 and he was brought to ED via ambulance. Lupu et al. Pain was decreased to 2/10.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content