This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
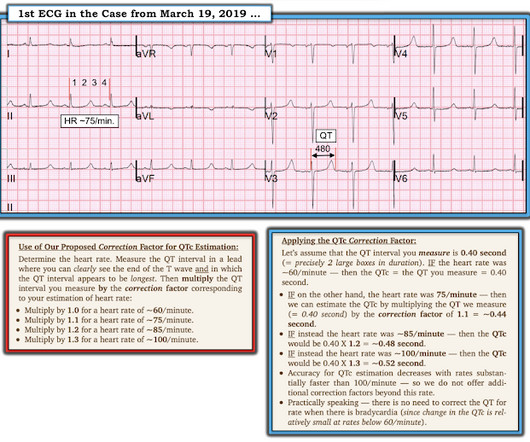
Bogossian et al. (1) Bogossian H, Frommeyer G, Ninios I, Hasan F, Nguyen QS, Karosiene Z, Mijic D, Kloppe A, Suleiman H, Bandorski D, et al. Among patients with left bundle branch block, T-wave peak to T-wave end time is prolonged in the presence of acute coronary occlusion. Then we can correct that modified QT for heart rate.
Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. For more on MINOCA — See My Comment in the November 16, 2023 post in Dr. Smith's ECG Blog ).
IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr. Smith's ECG Blog ). Why Was Cardiac Cath Negative for Coronary Disease?
Methodology: 3/5 Usefulness: 2/5 Ashburn NP, et al. Question and Methods: The authors completed preplanned subgroup analyses to determine if a 0-1 hour ultra-sensitive troponin […] The post Sensitivity Cardiac Troponin T Among Patients With Known Coronary Artery Disease appeared first on EMOttawa Blog. JAMA Cardiol.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Essentially, we are using the troponin assay to find patients with ACO who may be benefited by coronary interventions or risk factor modification. Cardiol Rev.
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] It’s judicious, then, to arrange for coronary angiogram.
Article: Branch KHR et al. Indication for emergency invasive coronary angiography or had coronary angiography within 1 hour of arrival. Known obstructive coronary artery disease or known coronary stent. References: Branch KHR et al. appeared first on REBEL EM - Emergency Medicine Blog. Resus 2023.
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT. Amsterdam et al. Alencar et al.
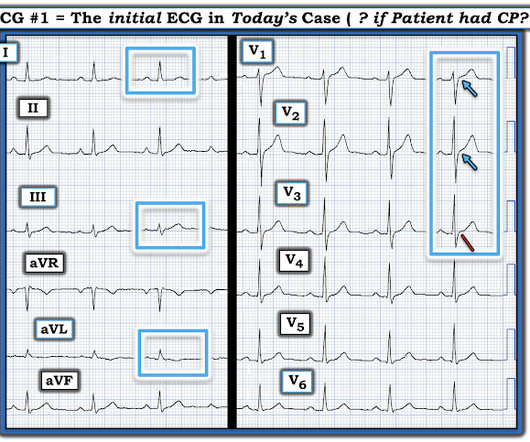
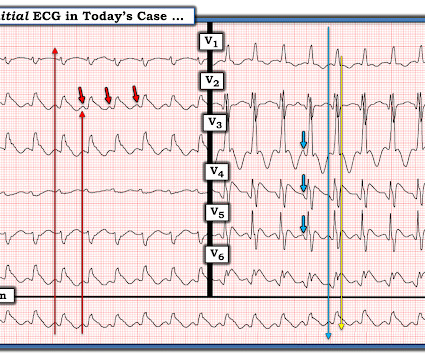
Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ). Figure-1: I've labeled the initial ECG in today's case.
Coronaries were clean. Not OMI with High Confidence Click here to sign up for Queen of Hearts Access We showed that the Queen of Hearts decreases false positive cath lab activations: 1) Published recently in Prehospital Emergency Care Baker PO et al. 2) To be presented at AHA conference in Chicago in 2 weeks: Sharkey SW et al.
Zeymer HT et al. References: Zeymer HT et al. PMID: 37634145 Post Peer Reviewed By: Anand Swaminathan, MD (Twitter/X: @EMSwami ) The post The ECLS-SHOCK Trial: ECPR in Infarct-Related Cardiogenic Shock appeared first on REBEL EM - Emergency Medicine Blog. bleeding, stroke, limb ischemia, and hemolysis). Control: 53.4%
Methodology: 3/5 Usefulness: 1/5 Georgiopoulos G, et al. The post Modification of the GRACE Risk Score for Risk Prediction in Patients With Acute Coronary Syndromes appeared first on EMOttawa Blog. JAMA Cardiol. Methods: Retrospective.
1] But there are multiple other abnormalities that make this ECG diagnostic of Occlusion MI, localized likely to the right coronary artery: 1. Systematic review and meta-analysis of diagnostic test accuracy of ST-segment elevation for acute coronary occlusion. Nikus et al. Kontos et al. Kontos et al. Bischof et al.
It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). Upon contrast injection of the LMCA, the patient deteriorated, as the LMCA was severely diseased and flow to all coronary arteries ( LAD, LCx and RCA ) was compromised. He was taken immediately to the cath lab.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
In fact, Kosuge et al. showed that among patients with either acute coronary syndrome or acute pulmonary embolism and negative T waves in the precordial leads (V1-V4), that inverted T waves in leads III and V1 were present in only 1% of patients with acute coronary syndrome and 88% of patients with pulmonary embolism. “The
Paper: Van de Werf, F et al. STREAM-2: Half-Dose Tenecteplase or Primary Percutaneous Coronary Intervention in Older Patients With ST-Segment-Elevation Myocardial Infarction: A Randomized, Open-Label Trial. References: Van de Werf, F et al. PMID: 37439219 Armstrong P et al.
A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. Lemkes JS, et al. Total coronary occlusion, if very brief, may have minimal infarction and yet be very dangerous. Am Heart J. 2000;139:430–436. Eur Heart J [Internet].
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. The original term " benign early repolarization" has fallen out of favor since the seminal paper by Haïssaguerre et al.
The proof of this is that only 5% of patients enrolled had acute coronary occlusion. Lemkes JS, Janssens GN, van der Hoeven NW, et al. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. We at Hennepin recently published this study Sharma et al. This study failed to do so. 5% vs. 58%!! 5% vs. 58%!!
The latest is Langlois-Carbonneau et al. But like many similar studies, the study was small (one year at one centre with no indication of the incidence of acute coronary occlusion), and it used as the gold standard the final cardiologist interpretation of the ECG - not the patient outcome! But according to Langlois-Carbonneau et al.,
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). From there you can link to other great websites (including Dr. Smith's ECG Blog) that provide multiple case studies of both subtle and overt hyperkalemia. link] [1] Zachary et al. 2] Costanzo, L. Physiology.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" She had a proven 100% Left Main occlusion No ST shift in aVR This pattern of RBBB/LAFB was also the most common pattern in Fiol et al.
I have here 38 cases of "Computer Normal" ECGs which were critically abnormal and the vast majority are missed acute coronary occlusions (Missed Acute OMI) and most were recognized by the physician. Of the Non-STEMI in our cohort, about 25% will actually have acute coronary occlusion. So this study is worthless and must be ignored.
This has been discussed many times before on this blog. In-depth discussion is beyond the scope of this blog. Serial ECGs enhance the diagnosis of acute coronary syndrome. Bigger et al. Sadowski ZP, Alexander JH, Skrabucha B, et al. Bigger JR Jr, Dresdale RJ, Heissenbuttel RH, et al. Leave it alone.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. References: Jaff MR et al. PMID: 21422387 Wan S et al. PMID: 15262836 Sharifi M et al. PMID: 27422214 Wang C et al. PMID: 19741062 Kucher N et al. PMID: 24226805 Piazza G et al. PMID: 26315743 Tapson VF et al. CHEST 2010.
In most cases, rather, the culprit is gross ischemia due to myocardial infarction, cardiomyopathy, or advanced coronary artery disease. Grauer on the Smith ECG Blog: [link] Take a deep dive into the management of TdP versus PVT with Dr. Smith: [link] [1] Callans, D. This finding might favor a diagnosis of ischemic-driven PVT.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So the patient had a transient acute coronary occlusion that spontaneously reperfused but is at risk for reocclusion. Deutch et al.
First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion. The new ACC expert consensus explains that: “STEMI ECG criteria on a standard 12-lead ECG alone will miss a significant minority of patients who have acute coronary occlusion. Take home 1.
He underwent coronary angiography which showed severe multivessel disease, and he agreed to proceed with workup for CABG. Additional review of ECG artifacts by Pérez-Riera et al ( Ann Noninvasic Electrocardiol 23:e12494, 2018 ) VT Artifact — by Knight et al: NEJM 341:1270-1274, 1999. The January 30, 2018 post — for PTA.
Below is the version standardized by PM Cardio app Meyers interpretation: Findings are specific for posterior (and also likely inferior) wall transmural acute infarction, most likely due to acute coronary occlusion (OMI). Most OMI have a peak Troponin T over 1000 ng/L [reference: Baro R et al. Clinical Cardiology 2019.
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. Figure 2-1 The V1 / V2 leads were appropriately placed in this circumstance, and dedicated followers of the Smith ECG Blog will instantly recognize the problem at hand.
Evidence regarding intervention to non-culprit plaques is mixed and beyond the scope of this blog post. Heitner et al. We have on many occasions in Dr. Smith's ECG Blog, highlighted the downside of indiscriminate use of morphine in patients who present with new ischemic CP ( C hest P ain ). DOI:10.1161/CIRCINTERVENTIONS.118.007305),
A Short Comment on PIRP and T Waves: Oliva et al found a strong association of myocardial rupture with postinfarction regional pericarditis. Another possible cause of pseudonormalization of T waves mentioned many times on this blog is the pseudonormalization caused by re-occlusion of an infarct related reperfused coronary artery.
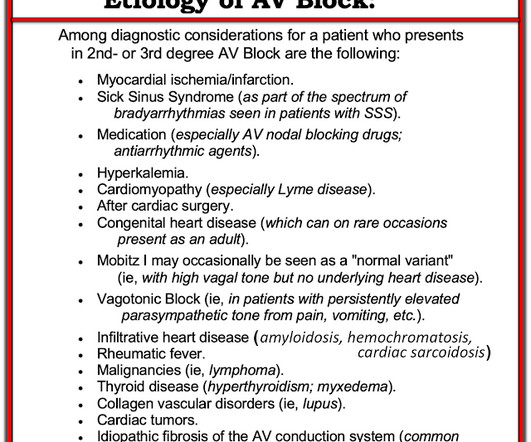
Even though the primary suspicion was not ischemic heart disease, a CT angiogram was performed, and it revealed normal coronary arteries. This ruled out coronary disease as the cause of conduction system disease. Most of the cases of AV block that we see in practice, are the result of underlying heart disease.
Dr. Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al. Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al.
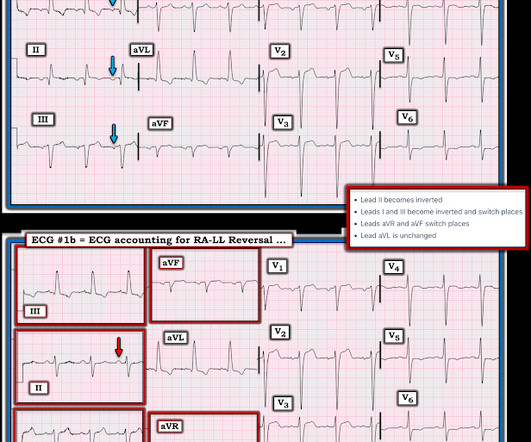
Therefore the impulse must have originated somewhere lower in the atria, perhaps near the coronary sinus. In the 500+ Comments I have written on Dr. Smith's ECG Blog since becoming an Associate Editor in 2018 — I do not believe we have had a case of RA-LL lead reversal. Complete heart block is the state of the AV node.
I have posted previous such cases, but in searching my own blog, I could not find them. The case I presented in My Comment to that March 9, 2020 post showed a patient with this pattern — who on cath had no more than minimal coronary disease. It would be a good topic for study. Smith adds to our knowledge of this syndrome.
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published. P.S.: Our September 3, 2020 post features Dr.
Background: Historically, we have treated acute coronary syndrome with supplemental oxygen regardless of the patient ’ s oxygen saturation. More recent evidence, however, demonstrates that too much oxygen could be harmful ( AVOID Trial ) by causing coronary vasoconstriction and increasing oxidative stress. Low O2 protocol: 3.1%
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content