This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Reference: Snyder BD, Van Dyke MR, Walker RG, et al. Reference: Snyder BD, Van Dyke MR, Walker RG, et al. You continue with compressions and defibrillations and your partner places an advanced airway. Association of small adult ventilation bags with return of spontaneous circulation in out of hospital cardiac arrest.
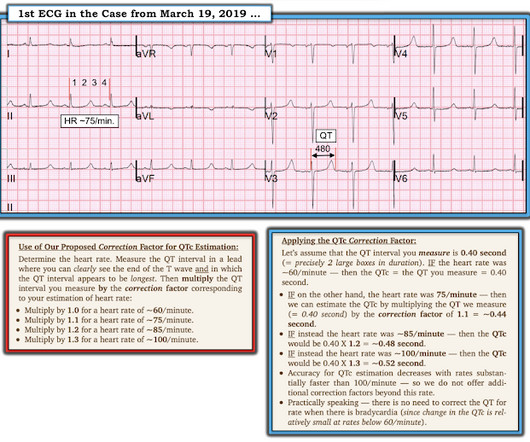
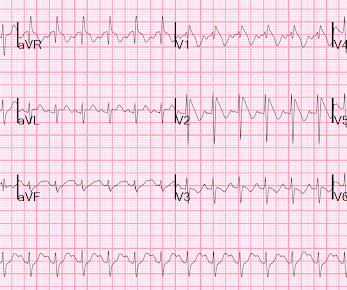
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. Lemkes JS, Janssens GN, van der Hoeven NW, et al. We at Hennepin recently published this study Sharma et al. Figure-1: I've labeled the initial ECG in today's case ( recorded after successful defibrillation ). 5% vs. 58%!!
Josh Kimbrell, NRP @joshkimbre Judah Kreinbrook, EMT-P @JMedic2JDoc This is the first installment of a blog series showing how transcutaneous pacing (TCP) can be difficult, and how you can improve your skills. The University of Maryland found that capture occurred in only 42-78% of patients, dependent on pad positioning (Moayedi et al, 2022).
Bogossian et al. (1) Bogossian H, Frommeyer G, Ninios I, Hasan F, Nguyen QS, Karosiene Z, Mijic D, Kloppe A, Suleiman H, Bandorski D, et al. For more on Torsades de Pointes vs PMVT See My Comment in the October 18, 2023 post and the September 2, 2024 post in Dr. Smith's ECG Blog ). Heart Rhythm [Internet]. 2014;11:22732277.
Background Information: Double external defibrillation (DED) is an intervention often used to treat refractory ventricular fibrillation (RVF). This procedure involves applying another set of pads attached to a second defibrillator to a patient and shocking them in hopes of terminating the rhythm. N Engl J Med.
He required multiple defibrillations within a period of a few hours. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. Some episodes of PMVT would terminate spontaneously — but on many occasions, the PMVT degenerated to VFib, requiring defibrillation.
Article: Branch KHR et al. Known cardiac defibrillator. References: Branch KHR et al. appeared first on REBEL EM - Emergency Medicine Blog. In theory, rapid identification of the underlying cause should improve outcomes by allowing clinicians to tailor management. Resus 2023. Pre-existing DNR order. Resus 2023.
He underwent further standard resuscitation EXCEPT that we applied the Inspiratory Threshold Device ( ResQPod ) AND applied Dual Sequential Defibrillation (this simply means we applied 2 sets of pads, had 2 defib machines, and defibrillated with both with only a fraction of one second separating each defibrillation.
This episode self terminated before defibrillation was possible. See Costagliola et al — Ann Clin Transl Neurol 8(7): 1557-1568, 2021 — for more on the complex "Brain-Heart Interaction" in Epilepsy ). This run of TdP is initiated by a PVC — but it then self-terminates. Discussion : The patient in today’s case presented with "seizures".
But artifact is "alive and well" — and learning to recognize it will amaze many of your colleagues ( and may serve to avoid an unnecessary defibrillation or two ). Additional review of ECG artifacts by Pérez-Riera et al ( Ann Noninvasic Electrocardiol 23:e12494, 2018 ) VT Artifact — by Knight et al: NEJM 341:1270-1274, 1999.
Two hours later , the patient returned to this same urgent care facility with worsening chest pain, and this ECG was performed: While getting another ECG, the patient suffered cardiac arrest: After multiple defibrillations, ROSC was achieved with ongoing "STEMI". Most OMI have a peak Troponin T over 1000 ng/L [reference: Baro R et al.
Adapted from Dr. Smith’s EKG Blog. Defibrillator pads are placed and you give 2 g IV magnesium over ten minutes. Figure 3/ Adapted from Wilde et al. A complete approach to treating cLQTS can be found in Wilde et al 2. An ECG is performed and is shown below: Figure 1. The patient is awake and protecting her airway.
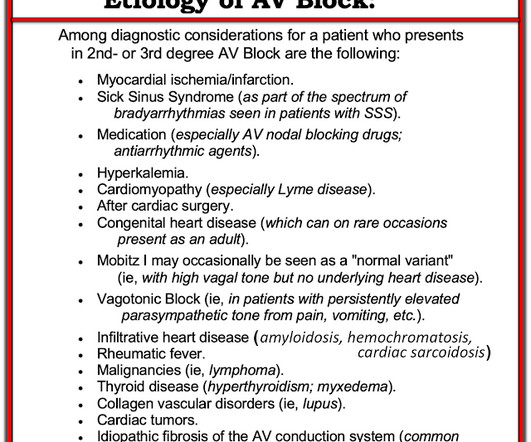
She was given CRT-D (Cardiac Resynchronization Therapy-Defibrillator). Learning points: == MY Comment , by K EN G RAUER, MD ( 1/15 /2024 ): == Today's case by Dr. Nossen differs from other cases of AV block we have published over the years in Dr. Smith's ECG Blog — in that the cause of AV block turned out to be CS ( C ardiac S arcoidosis ).
Background: There are only two interventions that have been proven in the medical literature to improved outcomes in cardiac arrest: high-quality CPR and early defibrillation. Article: Moore JC et al. References: Moore JC et al. It is imperative that we continue to look at ways to improve cardiac arrest resuscitation.
After resuscitation and defibrillation , there were no more episodes of TdP. Below is the patient’s 12 lead ECG following defibrillation. Most Torsades is the result of a pause-dependent effect that predisposes to development of the malignant arrhythmia ( Dohadwala et al — Heart Rhythm Case Rep 3(2):115-119, 2017 ).
ECG 2 Especially in the context of the first ECG, readers of this blog will readily appreciate the ST elevations and hyperacute T waves in II, III, aVF, V6, and to a lesser extent V5. As discussed on this blog many times before, proportionality is key to the diagnosis of OMI by ECG. [link] I also texted the ECG to Dr. Smith.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She was immediately intubated during continued compressions, then underwent a 9th defibrillation, which resulted in an organized rhythm at 42 minutes after initial arrest. see below).
She was defibrillated and resuscitated. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Lindahl et al. From Gue at al. Lindahl B, Baron T, Erlinge D, et al. Upon arrival to the emergency department, a senior emergency physician looked at the ECG and said "Nothing too exciting."
The patient was put on Extracorporeal Life Support in the ED 3 hours after initial resuscitation, the core temp was 30° C and the patient was defibrillated with a single attempt. Rituparna et al — as well as Chauhan and Brahma ( Int. On arrival, CPR was continued and core temperature was measured at 18° C (64.4° This is an Osborn wave.
Meyers et al. Aslanger et al. Lemkes et al. Bergmark et al. There was 100% proximal LAD occlusion, EF was 55% with severe hypokinesis to mid-distal septum and apex. First troponin I was 150 ng/L (normal <26 in males and <16 in females) and peak was 7,500. Int J Cardiol Heart Vasc 2021 2. Eur Heart J 2018 4.
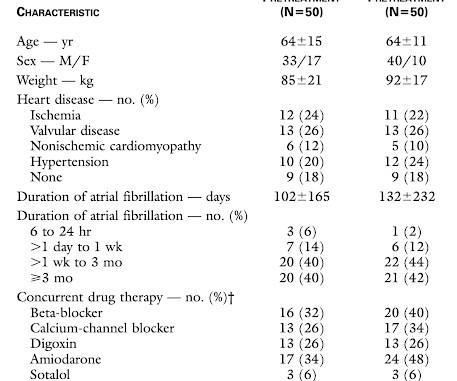
We examined the effect of ibutilide, a class III antiarrhythmic agent, on the energy requirement for atrial defibrillation and assessed the value of this agent in facilitating cardioversion in patients with atrial fibrillation that is resistant to conventional transthoracic cardioversion.
Armstrong et al. During angiogram in the cath lab, the patient suffered two episodes of ventricular fibrillation for which he was successfully defibrillated. We have tried to study it before, only to find that we cannot obtain enough cases of OMI with simultaneous high voltage in the leads with OMI findings, to study it.
In the largest study looking at this topic by Mizusawa et al., Recently the rate of true arrhythmic events related to fevers in the classic Brugada Type 1 syndrome was explored by Michowitz et al. 88 patients with fever induced Brugada Type 1 ECG changes without history of syncope or VF/VT were analyzed. There was a 0.9%
She was never seen to be in ventricular fibrillation and was never defibrillated. Kurkciyan et al. Kurkciyan et al., Medics found her apneic and pulseless, began CPR, and she was found to be in asystole. With ventilations and epinephrine, she regained a pulse. BP gradually rose. Of these, ischemic ST depression was found in 52%.
Excerpted from Vutthikraivit et al: Acta Cardiol Sin 34:267-277, 2018 ). == Distinction is made between 2 types of Brugada ECG patterns: A B rugada - 1 ECG pattern — shows ≥2 mm coved ST elevation with sharp downslope plus T wave inversion in ≥2 anterior leads. Cardioversion/defibrillation. Acute febrile illness. Hypothermia.
At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. He was given amiodarone and lidocaine load and drip and K and Mg drips.
the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. Here are other posts on hyperK, large calcium doses for hyperK, and ventricular tachycardia in hyperK Weakness, prolonged PR interval, wide complex, ventricular tachycardia Very Wide and Very Fast, What is it? How would you treat? Medicine (Baltimore) 1981;60:339-54].
Bayes de Luna, A et al. This is based on the Sieira et al, 2017, risk calculator , which gives a borderline risk score (2). An EP study might be helpful in symptomatic patients (Sroubek et al., Current electrocardiographic criteria for diagnosis of Brugada pattern: a consensus report. J Electrocardiology 45 (2012):433-442.
After epinephrine, atropine, and defibrillation x 2, there was a return of pulses. Plummer D et al. A 65 yo woman had felt ill for 36 hours, had seen her MD but without undergoing a cardiac evaluation. She collapsed and 911 was called; she was found pulseless. Exact rhythm during arrest is uncertain.
In this case, you should get a second defibrillator and perform double sequential external defibrillation (DSED). Simply attach a second defibrillator as shown in the diagram below and deliver max shocks from both devices simultaneously. Many similar cases have been featured on the blog.
This is the shock coil and identifies this device as a defibrillator. CRT-D is cardiac resynchronization therapy with defibrillation capability, like the CXR above. CRT-P is cardiac resynchronization therapy with pacing only, without the ability to defibrillate. Kaye et al. Canepa-Anson et al.
Although we lack details of events that followed Dr. Smith makes the key point that had this arrest witnessed by the medic team been the result of an acute cardiac event ( therefore, presumably VT or VFib ) prompt defibrillation by on-the-scene medics would most probably have resuscitated her.
Essentially, to put this blog to rest You will treat the patient the same as any other patient. With that being said, the manufacturers say that CPR, medications, Defibrillation, Cardioversion, and Anything you would normally do are OKAY. We still defibrillate ventricular fibrillation just as we would any other patient.
The intricacies of the different classes of antiarrhythmics and their mechanism of action extend beyond the scope of this blog. I list below links to other cases of idiopathic VT from Dr Smith's ECG blog. Try a different kind of antiarrhythmic. This is what was done in today's case. 2022, September 2) [2] Ward, R. Van Zyl, M., &
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content