This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
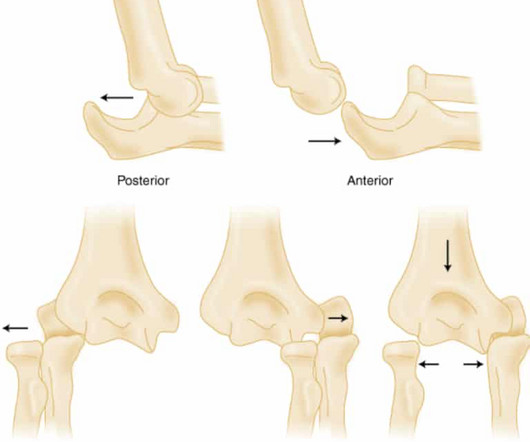
1998 Jan-Feb;6(1):15-23. PMID: 32644703 Robinson PM, Griffiths E, Watts AC. 2017 Jul;9(3):195-204. PMID: 29681420 Gottschalk HP, Eisner E, Hosalkar HS. 1999 Jan;13(1):58-9. Commentary on an article by Marc Schnetzke, MD, et al.: “Determination of Elbow Laxity in a Sequential Soft-Tissue Injury Model.
mental status, urine output, capillary refill) is more important than an actual goal PERMISSIVE HYPOTENSTION IN PTS WITH TBI Brotfain E et al. mental status, urine output, capillary refill) is more important than an actual goal PERMISSIVE HYPOTENSTION IN PTS WITH TBI Brotfain E et al. Richards JE et al.
I agree, however: 1) I don't think you can get a good enough ech o without bubble contrast. 3) E cho is another step that takes time. I had only 9 false positives but I missed 2 OMI. 2) To be presented at AHA conference in Chicago in 2 weeks: Sharkey SW et al. 2) You need to be just as expert at echo as I am at the ECG.
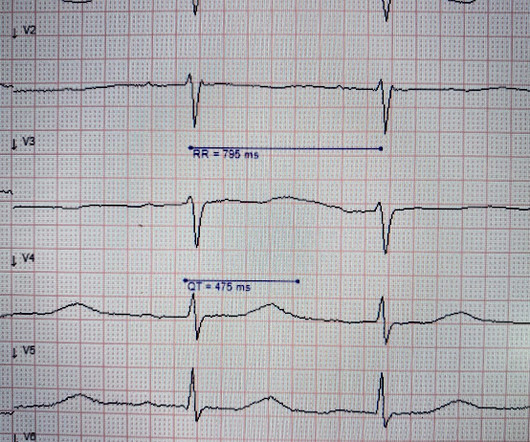
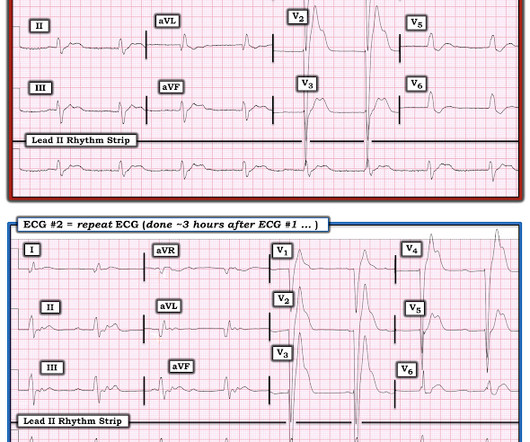
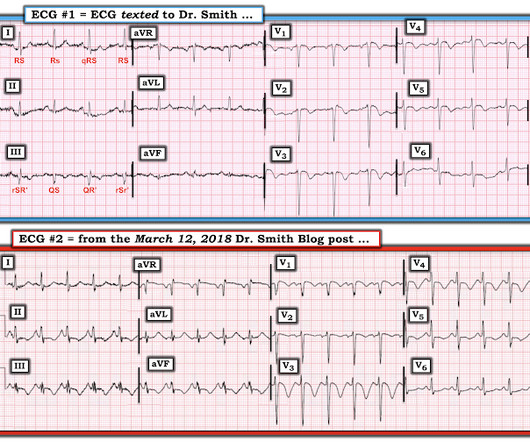
Here is lead I from ECGs 1 and 2 shown side-by-side to highlight the change in axis from borderline right to completely normal. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ).
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Challenge QUESTION: The relative change in T-QRS-D is not the only thing that changes during period of time that passed between recording of the 2 ECGs shown in Figure-1.
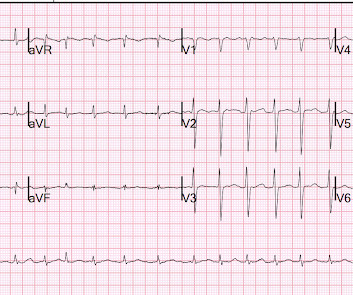
ECG #1 Interpretation: ECG #1 shows sinus rhythm at a heart rate of 77 bpm. Following more detailed questioning — it turned out the patient had started taking 9 different herbal remedies to ease lethargy and unspecific neurological symptoms. For clarity in Figure-1 — I've reproduced the initial ECG in today's case.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chest pain onset around 9 PM the evening prior. ECG 1 What do you think? Grines, C.
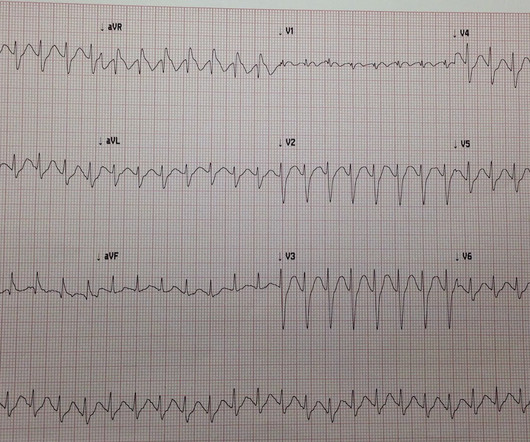
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. C Examination notable for diaphoresis, 1+ bilateral lower extremity edema, regular heart rate and rhythm, and no signs of respiratory distress with normal breath sounds. In fact, Kosuge et al. In fact, Kosuge et al.
Article: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM. Guideline-based and restricted fluid resuscitation strategy in sepsis patients with heart failure: A systematic review and meta-analysis [published online ahead of print, 2023 Aug 9]. Am J Emerg Med. 2023;73:34-39. Results: 26,069 studies met initial inclusion criteria.
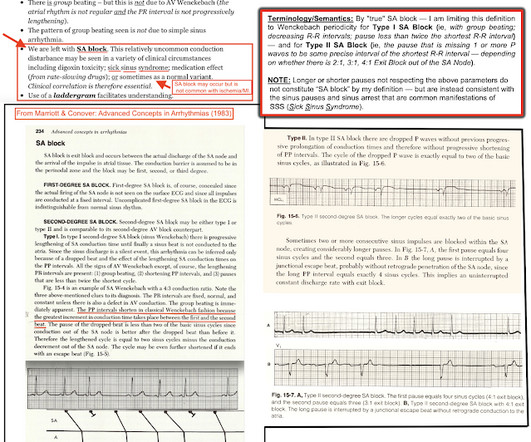
R waves 6 through 9 have no preceding P waves and are suspiciously regularly spaced. Depolarization wavefronts exit the sinus node through one or several sinoatrial conduction pathways (SACP) as seen in the histology section below taken from Li et al. Impulses E, F, G, H, and I were blocked. This is consistent with sinus rhythm.
1, 2 Its occurrence often portends worse outcomes in intubated patients, whose projected hospital course was already tenuous. 1, 4, 6 The overall incidence of VAP is somewhere around 5%-40% of all intubated patients, depending on the study and country from which it is reported. 4, 8 Paper: Dahyot-Fizelier, C.,
Initial vital signs include: NIBP 99/58 HR 150-160 (trend) RR 10 (spontaneous, but shallow) SpO2 86 (RA) BBS CTA The initial rhythm strip is attached: Figure 1 There is a wide complex tachycardia of varying morphology, amplitude, and R-R cycle length. A prominent vertical scar, however, is noted at the sternum.
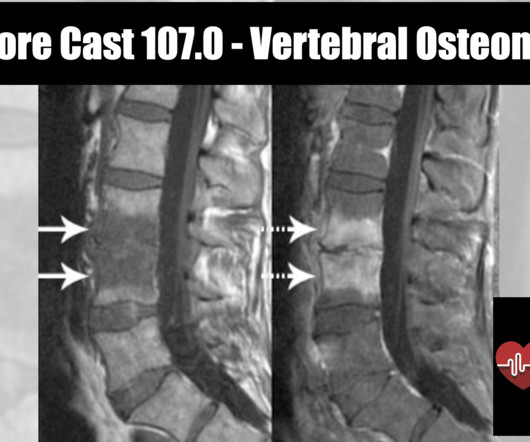
Epidemiology 1 to 2.4 cases per 100,000 people ( Zimmerli 2010 ) More common in males with M:F of 3:1 Rate is also increasing due to increased number of spinal procedures Typically affects adults, with most cases occurring in patients over 50 years old. Other pathogens include: E. PMID: 26316526 Boody B, et al.
Article: Arvig MD, Lassen AT, Gæde PH, et al. What They Did: Design: Randomized, controlled, blinded-outcome trial Sites: Three emergency departments in Denmark Duration: October 9, 2019 to May 26, 2021. The first evaluation of the patient was to be done within 1 hour of arrival to ED (Including the first POCUS). Emerg Med J.
CT head without contrast 1 is performed and reveals the following: Question: What is the diagnosis? Rosh Review Website Link Further Reading: FOAMed: [link] [link] [link] [link] [link] [link] [link] References : Turi B, Smith D, Kusel K, et al. Updated November 9, 2023. link] Sharma R, Gaillard F, Bell D, et al.
2024 Oct 9. You can find more details in the full blog post. There were no differences in survival (12% with IO vs 10% with IV) or neurologically intact survival (9% vs 8%). 2024 Nov 1. Restrictive vs Liberal Transfusion Strategy in Patients With Acute Brain Injury: The TRAIN Randomized Clinical Trial. doi: 10.1001/jama.2024.20424.
No significant differences in heart rate 1 minute after cardioversion were observed between the three groups. References: Appelboam A, Reuben A, Mann C, Gagg J, Ewings P, Barton A, et al. 2010;17(1):44-49. Duration of Antiarrhythmic Effect: MVM group: 35.44 seconds (SD = 7.73) Adenosine group: 24.24 seconds (range: 22.5,
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. Patients that develop a Type 1 pattern without any precipitating or provoking factors have a risk of SCD of 0.5-0.8% per year incidence of SCD in this cohort [1].
Features Urticaria and pruritis Rapid onset (1-2 hours) IgE Dependent (Type I Hypersensitivity) Reactions An allergen cross-links two or more IgE molecules on mast cells or basophils and initiates a signal cascade leading to degranulation. PMID 25629740 Hassen GW et al. PMID 23062323 Kostis JB et al. Zuraw et al.
This blog is an example of exactly that. While transporting to the emergency department, the patient’s mother informed me that PDCD affects less than 1 in 50,000 individuals and is more common in males than females. 6. Giribaldi G, Doria-Lamba L, Biancheri R, Severino M, Rossi A, Santorelli FM, et al. Always look it up!
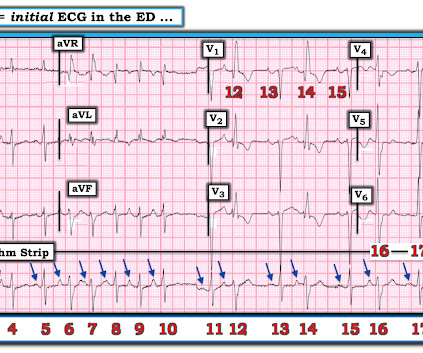
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiac arrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. Figure-1: The initial ECG in today's case — obtained after ROSC.
Post cath ECG: Now there are hyperacute T-waves again, and recurrent ST depression in V2 This ECG would normally diagnostic of OMI until proven otherwise No further troponins were measured, but it looks like there is recurrent OMI Next day: A CT Coronary Angiogram was done (CTCA) CARDIAC MORPHOLOGY AND FUNCTION: 1. IMPRESSION: 1.
Article: Marx T, Joly LM, Parmentier AL, et al. Sites: Investigators recruited patients at 31 French emergency departments at university and nonuniversity hospitals Duration : June 1, 2009 to March 31, 2015. Recurrence of pneumothorax within 1 year. Panacek, E. Cochrane Database of Systematic Reviews 2017, Issue 9.
To me, it was clearly atrial flutter with 1:1 conduction. Continue Eliquis 5mg BID, should be continued for 3 months == MY Comment , by K EN G RAUER, MD ( 9/18 /2024 ): == I found the following aspects of today's case of special interest. Why did Dr. Smith immediately say the rhythm was AFlutter with 1:1 AV conduction?
Over the last 1 week, her exertional chest pain became worse both in intensity and triggering threshold. link] Shvilkin et al. By contrast with today's case — I offer this tracing from a 60-year old woman with dyspnea and the ECG in Figure-1 showing LBBB conduction every-other-beat. is diagnostic of cardiac memory.
Article: Rossi N et al. Investigators enrollend 660 patients in 9 years in 5 EDs; or approximately 6 patients per month; or 1 patient per /month for each ED. The inclusion of p-values in Table 1 might lead to misinterpretation or improper use of statistical significance. Am J Emerg Med.
This was a very complex case and the details are too much for an ECG Blog, but suffice it to say that, s hortly thereafter, the patient had an asystolic arrest and was resuscitated. Learning Points: 1. For clarity in Figure-1 — I've reproduced and put these first 2 ECGs together. Figure-1: The first 2 tracings in today's case.
1-6 We now have the Community-Acquired Pneumonia: Evaluation of Corticosteroids (CAPE COD) Trial. Paper: Dequin P, Meziani F, Quenot J, et al. Patients admitted to the ICU with severe community-acquired pneumonia were randomized in a 1:1 ratio to receive hydrocortisone or a placebo. N Engl J Med. 2023;388(21):1931-1941.
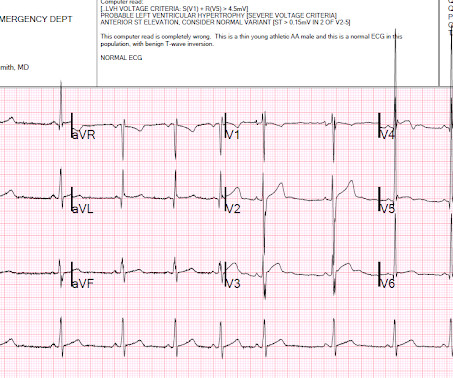
After having learned about benign T wave inversion pattern years ago on this blog, and having seen many cases on this blog and in my practice since then, I instantly recognize this as BTWI, a fairly common normal variant. see below for more info on this) 1. POINT # 2: The E CG F indings C hanged !
4 important features that indicate acute right hear strain: 1. Kosuge et al. In this study, (quote) "negative T waves in leads III and V 1 were observed in only 1% of patients with ACS compared with 88% of patients with APE (p less than 0.001). Witting et al. Finally, Stein et al. Tachycardia (or nearly) 2.
Previously, I wrote a blog on pre-oxygenation, referencing my personal “weapon of choice” as chosen from the 7 Ps of RSI. But, putting them both into one blog would make for a read far too long to maintain even my attention span (which honestly is pretty short). And according to a paper from Russotto et al.
Read More REBEL EM: The Ketorolac Analgesic Ceiling References Irizarry E et al. PMID: 34133820 Arora S et al. Can J Emerg Med 2007; 9(1): 30-2. PMID: 17391598 Wright JM et al. PMID: 7618770 Neighbor ML et al. PMID: 9492131 Mixter CG et al. PMID: 9565125 Qureshi I et al. 2019; 36: 401-6.
The pattern of STE and STD reminded us of Brugada Type 1 morphology. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. Patients that develop a Type 1 pattern without any precipitating or provoking factors have a risk of SCD of 0.5-0.8% per year incidence of SCD in this cohort [1].
But these cases show the potential dangers of delayed recognition and treatment of inferior reperfusion Take away 1. ECG’s can be labeled as ‘normal’ by the computer (and confirmed by cardiology) even with diagnostic signs of occlusion or reperfusion References 1. Backus BE, Six AJ, Kelder JC, et al. JAMA Intern Med 2019 9.
The data in the paper by Rangel et al. Vittinghoff, E. Metoprolol and atenolol are overwhelmingly beta-1 cardioselective. Beta-1 blockade decreases inotropy and chronotropy and has no vasoconstrictive effects. is intuitive, and not surprising. style='mso-element:field-begin'> ADDIN EN.CITE Rangel 1853 1853 17 Rangel, C.
Article: Kumar M et al. 2020;71(1):235-246. Plt 37×10^9/L and 40×10^9/L, SOC and TEG, respectively) All patients enrolled had an upper endoscopy and verified the source of bleeding. Hepatology. Significant coagulopathy: INR > 1.8 Significant coagulopathy: INR > 1.8
Here they are: Learning Points: 1. 3–8 Shi et al. 7 These 3 studies, as well as 1 smaller meta-analysis, 6 and another small study, 8 make it clear that troponin is associated with increased severity and mortality in COVID when adjusted for multiple other variables. Sandoval Y, Smith SW, Sexter A, et al.
He had episodes of chest pain off and on all night, until about 1 hour prior to arrival when the pain became constant, crushing, 10/10 chest pain that radiated to both arms. Proven STEMI has an open artery in 19% to 36% of cases, depending on whether it is TIMI −1, −2, or −3 flow. 25] Stone et al found that 72% have TIMI 0 or 1 flow.
1 However, it is important to understand that death from hemoptysis is almost always due to hypoxia or asphyxiation (blood impedes gas exchange in the lungs, typically because of bleeding from high-pressure bronchial arteries into the lungs) as opposed to hemodynamic instability. 2021;42(1):145-159. Li H, Ding X, Zhai S, et al.
Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Raitt et al.) [and Armstrong et al.)], the presence of such well developed anterior Q-wave suggests completed transmural STEMI. 3) Oliva et al. (3) Armstrong PW et al. J Am Coll Cardiol 53(17):1503-9. Very unlikely.
There are 5 other rhythms that are irregularly irregular , though atrial fibrillation is by far the most common: 1. However, incorrect automated and physician overread interpretations are common and have been shown to adversely affect patient management [ 1 ]. Taggar et al. Hwan Bae et al. Among, 2447 ECGs, Mant et al.
Paper: Smith JA, Secombe P, Aromataris E. Only 1 RCT and 1 cohort study had only mechanically ventilated patients. However, this data was driven by a single small trial (Enderson et al.), References: Smith JA, Secombe P, Aromataris E. appeared first on REBEL EM - Emergency Medicine Blog. in ICC group, 5.8%
Read More REBEL EM: The Ketorolac Analgesic Ceiling References Irizarry E et al. PMID: 34133820 Arora S et al. Can J Emerg Med 2007; 9(1): 30-2. PMID: 17391598 Wright JM et al. PMID: 7618770 Neighbor ML et al. PMID: 9492131 Mixter CG et al. PMID: 9565125 Qureshi I et al. 2019; 36: 401-6.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content