This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
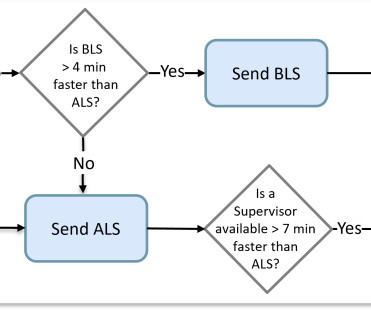
Some computer-aided dispatch (CAD) software did better than others by considering the average travel time of an actual route instead of allowing nearness to be determined by a straight-line distance. If available, the supervisor is added to effectively create an ALS transport ambulance.
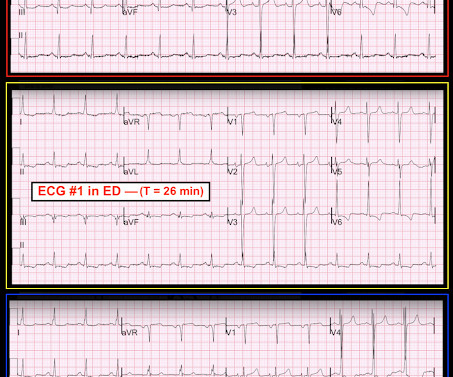
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System. 2021;23:187.
Date: June 30th, 2022 Reference: McGinnis et al. Date: June 30th, 2022 Reference: McGinnis et al. Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? AEM June 2022. Guest Skeptic: Dr. Corey Heitz is an emergency physician in Roanoke, Virginia. AEM June 2022.
Furthermore, there was no family history of early CAD, MI, or sudden cardiac death. He reported to EMS a medical history of GERD only. The physical exam was unremarkable for diaphoresis or pallor, and he denied any episodes of vomiting. 1] Driver, B. Posterior wall reperfusion T-waves: Wellens’ syndrome of the posterior wall. 3] Niu, T.,
Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example. CASE 1 A 45 y/o Male called 911 for new onset central chest discomfort, non-radiating, 5/10 pain scale, and without any vomiting, diaphoresis, or pallor. A 12 Lead ECG was recorded. References 1] Smith, S. 2] Driver, B. 3] Aslanger, E.,
EBM Update: Steroids in Severe CAP and CT in Post ROSC OHCA #1: Dequin PF, Meziani F, Quenot JP, et al; CRICS-TriGGERSep Network. Author Takeaway: No difference in mortality at 60 days with methylprednisolone vs. placebo in severe CAP #3: Wu JY, Tsai YW, Hsu WH, et al. Reyes LF, Garcia E, Ibáñez-Prada ED, et al. N Engl J Med.
Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram. Amsterdam et al. Alencar et al. Lupu et al. Herman, Meyers, Smith et al. link] References 1.
Increased risk in those with preexisting CKD, other risk factors for renal disease (HTN or CAD), and those on ACEIs/ARBs. Shetty R, Basheer FT, Poojari PG, et al. Wilding JPH, Batterham RL, Calanna S, et al; STEP 1 Study Group. Davies M, Færch L, Jeppesen OK, et al; STEP 2 Study Group. Front Endocrinol (Lausanne).
However, a smooth tapering of the mid-RCA was seen, highlighted in red below: How do we explain the MI if no sign of CAD was found? This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. A study by Hassan et al. Lobo et al. Lobo et al. The SCAD cases in Lobo et al.
The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. In the largest study looking at this topic by Mizusawa et al., Recently the rate of true arrhythmic events related to fevers in the classic Brugada Type 1 syndrome was explored by Michowitz et al.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Hayakawa A, Tsukahara K, Miyagawa S, et al. Written by Nathanael Franks MD, reviewed by Meyers, Smith, Grauer, etc. Am J Emerg Med.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. Conversely, Matetzky et al.
So I went to look at the chart and here is the history: This patient with no h/o CAD had a couple of episodes of chest pain during the day, then presented with one hour of substernal chest pain that had some reproducibility but also improved from 10/10 to 5/10 with nitroglycerine. Fesmire et al. Wang T, Zhang M, Fu Y, et al.
He had a family history of early CAD and occasional drug and tobacco use. Mawri S, Michaels A, Gibbs J, et al. It is not yet available, but this is your way to get on the list. link] Here is the history: A 30 yo man presented complaining of severe chest pain. The ECG was alarming to the ED physician who did indeed review it.
She had a proven 100% Left Main occlusion No ST shift in aVR This pattern of RBBB/LAFB was also the most common pattern in Fiol et al. See this paper by Widimsky et al, which shows the high association of RBBB, especially with LAFB, with LAD occlusion. Widimsky P et al. Knotts et al. Rokos IC, French WJ, Mattu A, et al.
A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. In the largest study looking at this topic by Mizusawa et al., She has not had a heart catheterization or after this event so the presence or absence of CAD is still unknown.
Late Gadolinium enhancement: Multifocal scarring of the septum (including RV septum), basal anterior wall and transmural mid inferior region scarring - a non-CAD hyperenhacement pattern. There is mild-moderate tricuspid valve regurgitation. Overall CMR findings are consistent with arrhythmogenic cardiomyopathy. RVEF 100 ml/m2.
Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? -- these are entirely different) Moderate single-vessel CAD.
She also had non-acute CAD of the left main (50%) and LCX (75%). Patel et al., Krucoff et al.) Patel et al. Krucoff et al. Schomig et al. Krucoff et al.) ) to disastrous consequences that may deteriorate before the patient can be rushed to the cath lab. They opened it. Initial troponin T was 0.46
A middle-aged male with h/o CAD and stents presented with typical chest pressure. See this paper by Widimsky et al, which shows the high association of RBBB, especially with LAFB, with LAD occlusion. Here is his ECG: The resident was alarmed at the "ST elevation in III with reciprocal ST depression in aVL" Are you alarmed?
As I met the paramedics and cath team in the lab, I was ready to see severe coronary disease (CAD), but the vessels were non-obstructive. Dobutamine may be preferred in patients without severe hypotension who have high vascular resistance. -- De Backer D et al. Taglieri N, Marzocchi A, Saia F, et al. Richard, C; et al.
Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. The criteria of Armstrong et al. One retrospective analysis by Armstrong et al. Armstrong EJ, Kulkarni AR, Bhave PD, et al. AT, Jaffa EJ, et al. Neuman Y, Cercek B, Aragon J, et al. Am J Emerg Med.
This study from Herzog et al (from our own Hennepin County Medical Center) included patients from a national registry and compared 3049 patients on dialysis admitted and eventually found to have acute MI compared with 534,395 patients not on dialysis admitted with an eventual diagnosis of acute MI. Herzog et al.
No family history of sudden cardiac death, cardiomyopathy, premature CAD, or other cardiac issues. There is a literature on this subject ( GGF van der Schoot et al: Neth Heart J 28(6):301-308, 2020 — and — Egred et al — Postgrad Med 81(962): 741-745, 2005 — to name just 2 reports ). No similar symptoms in the past.
He also had non-acute CAD of the RCA (50%) and LCX (50%). CLICK HERE — for a brief article by Rowlands et al that explains these concepts in more detail. Cardiology was called and the patient was taken for urgent catheterization with the time from ED arrival to cath about 1 hour and 45 minutes. Cath images: Before intervention.
He had significant history of CAD with CABG x5, and repeat CABG x 2 as well as a subsequent PCI of the graft to the RCA (twice) and of the graft to the Diagonal. the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. A late middle-aged man presented with one hour of chest pain. Most recent echo showed EF of 60%.
IIa C During hospital stay (after primary PCI) Either stress echo, CMR, SPECT, or PET may be used to assess myocardial ischaemia and viability, including in multivessel CAD. I C During hospital stay (after primary PCI) When echocardiography is suboptimal/inconclusive, an alternative imaging method (CMR preferably) should be considered.
Scattered other nonobstructive CAD. de Winter et al in N Engl J Med 359:2071-2073, 2008. Angiogram around 9am: Culprit lesion mid LAD 100% stenosis TIMI 0 TIMI 3 after PCI Severe apical dyskinesis, severe anteroapical akinesis. Figure-1: The de Winter T Wave Pattern , as first described by Robbert J.
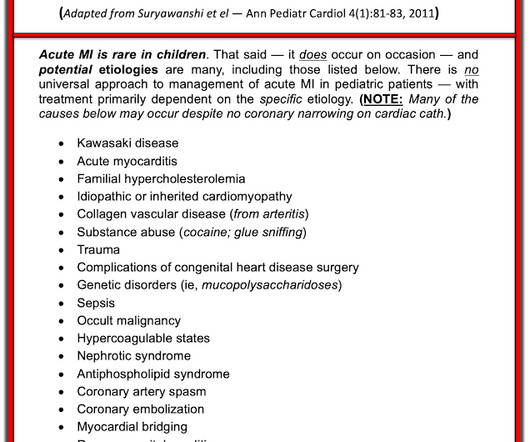
He did have a family history notable for early CAD. hematological disorder like sickle cell or antiphospholipid syndome, family history of CAD or hypercholesterolemia, prior history of vasculopathies such as Kawasaki Disease, MIS-C, prior cardiac surgery, etc.) He denied drug or alcohol use. mg/L and a normal WBC of 8.8. .-
He has a history of CHF, dilated cardiomyopathy, HTN, HLD and CAD. Isenhour JL, Craig S, Gibbs M, et al. For this box, please keep ventricular tachycardia (VTach) and supraventricular tachycardia with aberrancy (SVT with aberrancy) in your differential. This EKG comes from a 75-year-old male presenting with palpitations. Vereckei A.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content