This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Reference: McGinnis et al.
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT. Amsterdam et al. Alencar et al.
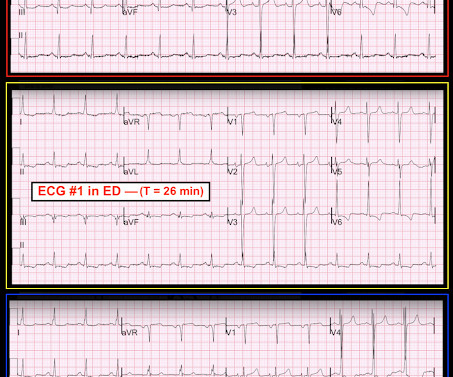
Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example. One cannot rely on this feature as a means of detecting changes – subtle, or dramatic – for volatile occlusive coronary thrombus. A 12 Lead ECG was recorded. Raw findings include Sinus Rhythm amidst an otherwise normal QRS.
Furthermore, there was no family history of early CAD, MI, or sudden cardiac death. Cardiology admitted him for observation with plans for next-day coronary angiogram. He reported to EMS a medical history of GERD only. The physical exam was unremarkable for diaphoresis or pallor, and he denied any episodes of vomiting. 1] Driver, B.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" She had a proven 100% Left Main occlusion No ST shift in aVR This pattern of RBBB/LAFB was also the most common pattern in Fiol et al.
The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA.
GLP-1 agonists are also associated with improved ejection fraction, coronary blood flow, and cardiac output while reducing the risk of cardiovascular events, infarction size, and all-cause mortality. Increased risk in those with preexisting CKD, other risk factors for renal disease (HTN or CAD), and those on ACEIs/ARBs. N Engl J Med.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The De Winter ECG pattern: morphology and accuracy for diagnosing acute coronary occlusion: systematic review. 2009;95:1701–1706.
Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. It can only be seen by IVUS.
I want all to know that, with the right mind preparation, and the use of the early repol/LAD occlusion formula, extremely subtle coronary occlusion can be detected prospectively, with no other information than the ECG. It is not a missed STEMI, but it is a missed coronary occlusion. Fesmire et al. Wang T, Zhang M, Fu Y, et al.
The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. In the largest study looking at this topic by Mizusawa et al., She has not had a heart catheterization or after this event so the presence or absence of CAD is still unknown.
No family history of sudden cardiac death, cardiomyopathy, premature CAD, or other cardiac issues. Repeat CT angio chest (not CT coronary, unclear what protocol) showed possible LAD aneurysm and thrombus. Acute coronary occlusion almost always occurs in patients who are well beyond their teenage years.
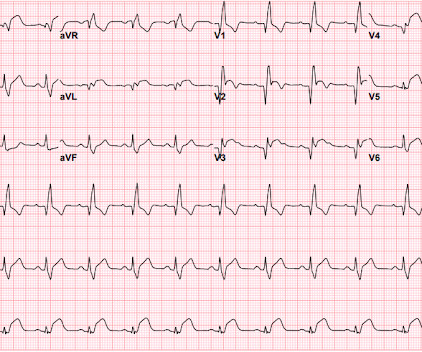
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. Conversely, Matetzky et al.
The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
He had a family history of early CAD and occasional drug and tobacco use. However, subtle coronary occlusion may be completely missed by the computer and called "normal." Mawri S, Michaels A, Gibbs J, et al. It is not yet available, but this is your way to get on the list. This one was not even so subtle!!! References : 1.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. Is there likely to be fixed coronary stenosis that led to demand ischemia during pneumonia? --Was See this paper by Widimsky et al, which shows the high association of RBBB, especially with LAFB, with LAD occlusion. This is a very common misread.
Late Gadolinium enhancement: Multifocal scarring of the septum (including RV septum), basal anterior wall and transmural mid inferior region scarring - a non-CAD hyperenhacement pattern. There is mild-moderate tricuspid valve regurgitation. Overall CMR findings are consistent with arrhythmogenic cardiomyopathy. RVEF 100 ml/m2.
Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. The criteria of Armstrong et al. LVH can mimic an acute anterior coronary occlusion (ACO) on the ECG. One retrospective analysis by Armstrong et al. Armstrong EJ, Kulkarni AR, Bhave PD, et al. J Emerg Med.
She also had non-acute CAD of the left main (50%) and LCX (75%). Patel et al., Krucoff et al.) Patel et al. Krucoff et al. Schomig et al. Krucoff et al.) ) to disastrous consequences that may deteriorate before the patient can be rushed to the cath lab. They opened it. Initial troponin T was 0.46
He also had non-acute CAD of the RCA (50%) and LCX (50%). This is a h igher - p revalence H istory for acute coronary disease. CLICK HERE — for a brief article by Rowlands et al that explains these concepts in more detail. Cath images: Before intervention. Before intervention with arrows demonstrating the area of occlusion.
This study from Herzog et al (from our own Hennepin County Medical Center) included patients from a national registry and compared 3049 patients on dialysis admitted and eventually found to have acute MI compared with 534,395 patients not on dialysis admitted with an eventual diagnosis of acute MI. Herzog et al.
This page summarises the most current recommendations for the management of acute coronary syndromes with persistent ST-segment elevations (i.e III A Primary percutaneous coronary intervention strategy Management Recommendation Level of evidence Primary PCI of the infarct related artery (IRA) is indicated.
He had significant history of CAD with CABG x5, and repeat CABG x 2 as well as a subsequent PCI of the graft to the RCA (twice) and of the graft to the Diagonal. the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. A late middle-aged man presented with one hour of chest pain. Most recent echo showed EF of 60%.
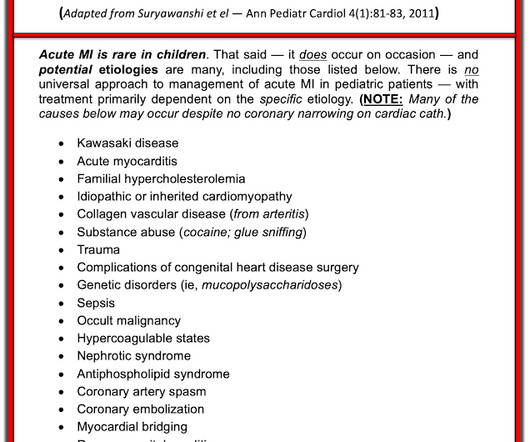
Acute coronary syndrome in a pediatric patient? He did have a family history notable for early CAD. hematological disorder like sickle cell or antiphospholipid syndome, family history of CAD or hypercholesterolemia, prior history of vasculopathies such as Kawasaki Disease, MIS-C, prior cardiac surgery, etc.)
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content