This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Date: June 30th, 2022 Reference: McGinnis et al. Date: June 30th, 2022 Reference: McGinnis et al. Case: You are working a shift in your local community emergency department (ED) when a 47-year-old male presents with chest pain. Background: Chest pain is one of the most common presentations to the ED. AEM June 2022.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. This case was sent by Amandeep (Deep) Singh at Highland Hospital, part of Alameda Health System. 2021;23:187.
Furthermore, there was no family history of early CAD, MI, or sudden cardiac death. 1] Here is the admitting ED ECG after cancellation of Code STEMI. The patient continued to verbalize cessation of symptoms while in the ED. He reported to EMS a medical history of GERD only. However, in this context (i.e. 1] Driver, B.
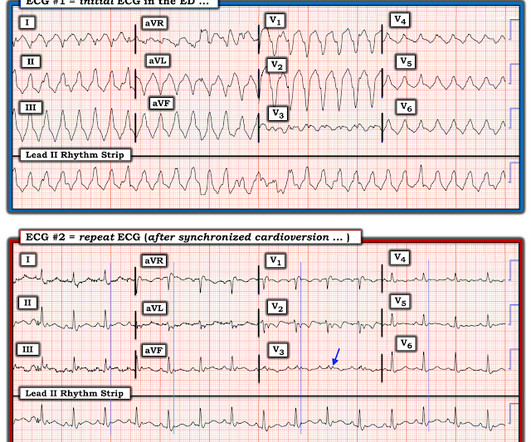
Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example. Here is the final ECG just prior to ED transfer. Attached below is the initial ED tracing upon hospital arrival, approximately 25 minutes after the prehospital ECG. A 12 Lead ECG was recorded. No serial ECG’s were recorded.
EBM Update: Steroids in Severe CAP and CT in Post ROSC OHCA #1: Dequin PF, Meziani F, Quenot JP, et al; CRICS-TriGGERSep Network. Author Takeaway: No difference in mortality at 60 days with methylprednisolone vs. placebo in severe CAP #3: Wu JY, Tsai YW, Hsu WH, et al. Reyes LF, Garcia E, Ibáñez-Prada ED, et al.
Despite otherwise normal vital signs, she was appropriately triaged to the critical care area of the ED. They are rare and hard to find in normal practice in the ED. She denied chest pain and denied feeling any palpitations, even during her triage ECG: What do you think? There is mild-moderate tricuspid valve regurgitation.
link] A 30 year-old woman was brought to the ED with chest pain. However, a smooth tapering of the mid-RCA was seen, highlighted in red below: How do we explain the MI if no sign of CAD was found? This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. A study by Hassan et al.
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. QOH Interpretation: The initial troponin I (older generation) at the first ED was barely positive at 0.06 In the largest study looking at this topic by Mizusawa et al., He denied chest pain or shortness of breath.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Hayakawa A, Tsukahara K, Miyagawa S, et al. Written by Nathanael Franks MD, reviewed by Meyers, Smith, Grauer, etc.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. Conversely, Matetzky et al.
This was my thought: if this patient presented to the ED with chest pain, then this is an LAD occlusion. Fesmire et al. Wang T, Zhang M, Fu Y, et al. Sorajja P, Gersh BJ, Cox DA, et al. Pride YB, Tung P, Mohanavelu S, et al. Marti D et al. See image below: Slow upstroke, fast downstroke. Asymmetric.
He had a family history of early CAD and occasional drug and tobacco use. The ECG was alarming to the ED physician who did indeed review it. Mawri S, Michaels A, Gibbs J, et al. It is not yet available, but this is your way to get on the list. link] Here is the history: A 30 yo man presented complaining of severe chest pain.
Smith and Meyers answer: First , LM occlusion is uncommon in the ED because most of these die before they can get a 12-lead recorded. She had a proven 100% Left Main occlusion No ST shift in aVR This pattern of RBBB/LAFB was also the most common pattern in Fiol et al. Widimsky P et al. Knotts et al. References 7.
She was asymptomatic at the time of this ECG recorded on arrival to our ED: What do you think? She also had non-acute CAD of the left main (50%) and LCX (75%). Patel et al., Krucoff et al.) Patel et al. Krucoff et al. Schomig et al. What will you do for this asymptomatic patient??? They opened it.
A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. In the largest study looking at this topic by Mizusawa et al., She has not had a heart catheterization or after this event so the presence or absence of CAD is still unknown.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. The patient arrived in the ED and had this ECG recorded: Interpretation? See this paper by Widimsky et al, which shows the high association of RBBB, especially with LAFB, with LAD occlusion. This is a very common misread.
Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? -- these are entirely different) Moderate single-vessel CAD.
His ED cardiac ultrasound (which is not at all ideal for detecting wall motion abnormalities, and is also very operator dependent for this finding) was significant for depressed global EF. In this study of dialysis patients with severe CAD, 77% had an abnormal resting EKG and the most common abnormality was LVH. Herzog et al.
The patient was brought directly to the cardiac catheterization lab for PCI, bypassing the ED. As I met the paramedics and cath team in the lab, I was ready to see severe coronary disease (CAD), but the vessels were non-obstructive. Taglieri N, Marzocchi A, Saia F, et al. Kosuge M, Ebina T, Hibi K, et al. Khot, MD; et al.
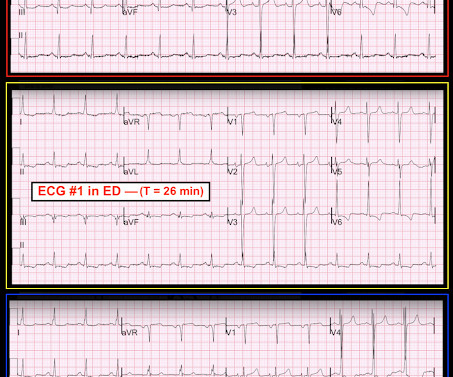
Cardiology was called and the patient was taken for urgent catheterization with the time from ED arrival to cath about 1 hour and 45 minutes. He also had non-acute CAD of the RCA (50%) and LCX (50%). I focus my att ention on the interpretation of the initial ED tracing ( = E CG # 1 in Figure-1 ).
Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. The criteria of Armstrong et al. One retrospective analysis by Armstrong et al. Armstrong EJ, Kulkarni AR, Bhave PD, et al. AT, Jaffa EJ, et al. Neuman Y, Cercek B, Aragon J, et al.
No family history of sudden cardiac death, cardiomyopathy, premature CAD, or other cardiac issues. There is a literature on this subject ( GGF van der Schoot et al: Neth Heart J 28(6):301-308, 2020 — and — Egred et al — Postgrad Med 81(962): 741-745, 2005 — to name just 2 reports ). No similar symptoms in the past.
He had significant history of CAD with CABG x5, and repeat CABG x 2 as well as a subsequent PCI of the graft to the RCA (twice) and of the graft to the Diagonal. Here is his ED ECG: There is obvious infero-posterior STEMI. the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. Most recent echo showed EF of 60%.
Cardiology refused to be the admitting physician because it was "NSTEMI", and forced the ED physician to admit the patient to the hospitalist. Of course, there was terrible boarding and the patient was considered non-emergent (NSTEMI), and so could not leave the ED for some time. Scattered other nonobstructive CAD.
He did have a family history notable for early CAD. An ECG was perfomed on arrival to our ED: NSR with ST elevation II,III, aVF with reciprocal depression in aVL Would you refer this pediatric patient for emergent PCI? He denied drug or alcohol use. The workup at the transferring hospital yielded elevated troponin I at 18.1
He has a history of CHF, dilated cardiomyopathy, HTN, HLD and CAD. Remember, from the ED point of view, if you are confronted with a wide complex regular tachydysrhythmia, assume VTach until proven otherwise! Isenhour JL, Craig S, Gibbs M, et al. This EKG comes from a 75-year-old male presenting with palpitations. Vereckei A.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content