This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
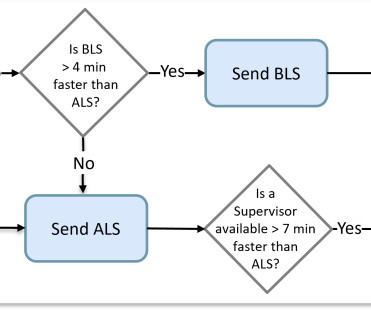
Some computer-aided dispatch (CAD) software did better than others by considering the average travel time of an actual route instead of allowing nearness to be determined by a straight-line distance. It was a matter of determining which crew was available closest to the scene. The idea here is to preserve this very limited resource.
Furthermore, there was no family history of early CAD, MI, or sudden cardiac death. A 56 y/o Male called 911 from his hotel room in the early morning hours after abruptly awakening from sleep with crushing chest discomfort and difficulty breathing. He reported to EMS a medical history of GERD only. He left AMA and is lost to follow-up.
The patient presented to an outside hospital An 80yo female per triage “patient presents with chest pain, also hurts to breathe” PMH: CAD, s/p stent placement, CHF, atrial fibrillation, pacemaker (placed 1 month earlier), LBBB. HPI: Abrupt onset of substernal chest pain associated with nausea/vomiting 30 min PTA. This was stented with a 2.25
Date: June 30th, 2022 Reference: McGinnis et al. Date: June 30th, 2022 Reference: McGinnis et al. Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? AEM June 2022. Guest Skeptic: Dr. Corey Heitz is an emergency physician in Roanoke, Virginia. AEM June 2022.
Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example. CASE 1 A 45 y/o Male called 911 for new onset central chest discomfort, non-radiating, 5/10 pain scale, and without any vomiting, diaphoresis, or pallor. A 12 Lead ECG was recorded. There is no dramatic change, or evolution. 2] Driver, B.
EBM Update: Steroids in Severe CAP and CT in Post ROSC OHCA #1: Dequin PF, Meziani F, Quenot JP, et al; CRICS-TriGGERSep Network. Author Takeaway: No difference in mortality at 60 days with methylprednisolone vs. placebo in severe CAP #3: Wu JY, Tsai YW, Hsu WH, et al. Reyes LF, Garcia E, Ibáñez-Prada ED, et al. N Engl J Med.
Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram. Amsterdam et al. Alencar et al. Lupu et al. Herman, Meyers, Smith et al. link] References 1.
Increased risk in those with preexisting CKD, other risk factors for renal disease (HTN or CAD), and those on ACEIs/ARBs. The effects of GLP-1 agonists are associated with the dose. Higher doses of GLP-1 agonists are associated with weight loss. Take for example semaglutide. Ozempic is utilized for DM2 in doses of 0.5, mg SQ every week.
The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. In the largest study looking at this topic by Mizusawa et al., Written by Pendell Meyers A man in his 70s with no cardiac history presented with acute weakness, syncope, and fever. There was a 0.9%
However, a smooth tapering of the mid-RCA was seen, highlighted in red below: How do we explain the MI if no sign of CAD was found? This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA. A study by Hassan et al. Lobo et al. This case occurred 10+ years ago.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Hayakawa A, Tsukahara K, Miyagawa S, et al. Written by Nathanael Franks MD, reviewed by Meyers, Smith, Grauer, etc. Am J Emerg Med.
Late Gadolinium enhancement: Multifocal scarring of the septum (including RV septum), basal anterior wall and transmural mid inferior region scarring - a non-CAD hyperenhacement pattern. There is clearly a wide complex tachcyardia (although the QRS duration is not far above 120msec). Or it could simply still be classic VT. RVEF 100 ml/m2.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. Conversely, Matetzky et al.
A formal echocardiogram was completed the next day and again showed a normal ejection fraction without any focal wall motion abnormalities to suggest CAD. In the largest study looking at this topic by Mizusawa et al., Schick is a PGY3 at the Brown Emergency Medicine Residency in Rhode Island. The article is edited by Smith.
She had a proven 100% Left Main occlusion No ST shift in aVR This pattern of RBBB/LAFB was also the most common pattern in Fiol et al. See this paper by Widimsky et al, which shows the high association of RBBB, especially with LAFB, with LAD occlusion. Widimsky P et al. Total LM occlusion can present with STE or STD in aVR.
So I went to look at the chart and here is the history: This patient with no h/o CAD had a couple of episodes of chest pain during the day, then presented with one hour of substernal chest pain that had some reproducibility but also improved from 10/10 to 5/10 with nitroglycerine. Fesmire et al. Wang T, Zhang M, Fu Y, et al.
He had a family history of early CAD and occasional drug and tobacco use. Mawri S, Michaels A, Gibbs J, et al. An ECG is recorded and the computer reads it as "normal". Do you want to see it? Or would you rather not be bothered? I'd rather be bothered. Here it is: Computer read: "Normal ECG" Aren't you glad that you looked at it?
She also had non-acute CAD of the left main (50%) and LCX (75%). Patel et al., Krucoff et al.) Patel et al. Krucoff et al. Back to the case: The providers recognized persistent ischemia and likely occlusion, and discussed this with cardiology who took the patient immediately for cath. They opened it. Heart 1996.
Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? -- these are entirely different) Moderate single-vessel CAD.
As I met the paramedics and cath team in the lab, I was ready to see severe coronary disease (CAD), but the vessels were non-obstructive. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
A middle-aged male with h/o CAD and stents presented with typical chest pressure. See this paper by Widimsky et al, which shows the high association of RBBB, especially with LAFB, with LAD occlusion. Here is his ECG: The resident was alarmed at the "ST elevation in III with reciprocal ST depression in aVL" Are you alarmed?
No family history of sudden cardiac death, cardiomyopathy, premature CAD, or other cardiac issues. No similar symptoms in the past. No prior exertional complaints of chest pain, dizziness, lightheadedness, or undue shortness of breath. He denied headache or neck pain associated with exertion. No further troponins were measured. Pericarditis?
This study from Herzog et al (from our own Hennepin County Medical Center) included patients from a national registry and compared 3049 patients on dialysis admitted and eventually found to have acute MI compared with 534,395 patients not on dialysis admitted with an eventual diagnosis of acute MI. Herzog et al. What can we learn?
Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. The criteria of Armstrong et al. One retrospective analysis by Armstrong et al. There is ST elevation, but also high voltage (though the high voltage is NOT in the leads with worrisome STE, rather, it is in aVL).
He also had non-acute CAD of the RCA (50%) and LCX (50%). CLICK HERE — for a brief article by Rowlands et al that explains these concepts in more detail. Cardiology was called and the patient was taken for urgent catheterization with the time from ED arrival to cath about 1 hour and 45 minutes. Cath images: Before intervention.
He had significant history of CAD with CABG x5, and repeat CABG x 2 as well as a subsequent PCI of the graft to the RCA (twice) and of the graft to the Diagonal. the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. A late middle-aged man presented with one hour of chest pain. Most recent echo showed EF of 60%.
I C Blood samples Management Recommendation Level of evidence Serum biomarkers of myocardial infarction ( troponin ) should be sampled as early as possible without delaying reperfusion therapy. I C Symptom relief Symptom Management Recommendation Level of evidence Hypoxia Oxygen is indicated if SaO2 < 90% or PaO2 < 60 mmHg.
Scattered other nonobstructive CAD. de Winter et al in N Engl J Med 359:2071-2073, 2008. Angiogram around 9am: Culprit lesion mid LAD 100% stenosis TIMI 0 TIMI 3 after PCI Severe apical dyskinesis, severe anteroapical akinesis. When you register on the app, you need to say you are from a supported country in the EU.
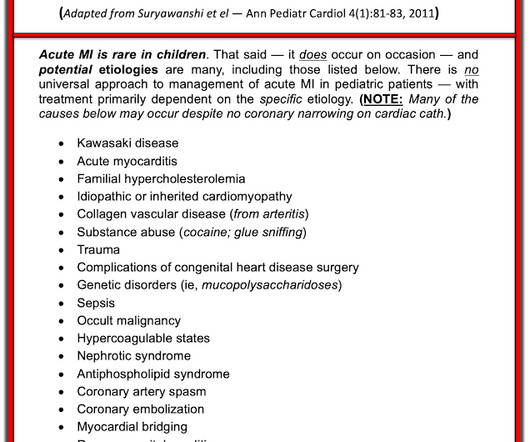
He did have a family history notable for early CAD. hematological disorder like sickle cell or antiphospholipid syndome, family history of CAD or hypercholesterolemia, prior history of vasculopathies such as Kawasaki Disease, MIS-C, prior cardiac surgery, etc.) He denied drug or alcohol use.
He has a history of CHF, dilated cardiomyopathy, HTN, HLD and CAD. Isenhour JL, Craig S, Gibbs M, et al. These are very commonly encountered in the emergency department, so being able to correctly identify the rhythm is extremely important. Lets dive in! This EKG comes from a 75-year-old male presenting with palpitations. Vereckei A.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content