This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation. Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients.
Article: Branch KHR et al. Indication for emergency invasive coronary angiography or had coronary angiography within 1 hour of arrival. Known obstructive coronary artery disease or known coronary stent. References: Branch KHR et al. Advanced imaging post-arrest is a possible modality to achieve this end.
Zeymer HT et al. Did they get bystander CPR? References: Zeymer HT et al. The benefits of this strategy may be outweighed by the risk of the device-related complications (i.e. bleeding, stroke, limb ischemia, and hemolysis). The evidence for this practice has been sparse until now. Control: 53.4% D ECLS: 18.2% Control 8.7%
Paper: Van de Werf, F et al. STREAM-2: Half-Dose Tenecteplase or Primary Percutaneous Coronary Intervention in Older Patients With ST-Segment-Elevation Myocardial Infarction: A Randomized, Open-Label Trial. References: Van de Werf, F et al. PMID: 37439219 Armstrong P et al.
Here is the case: Report from EMS was witnessed syncope, his son did CPR, but the patient had pulses when EMS arrived. The fact that this is syncope makes give it a far lower pretest probability than chest pain, but it was really more than syncope, as the patient actually underwent CPR and had hypotension on arrival of EMS.
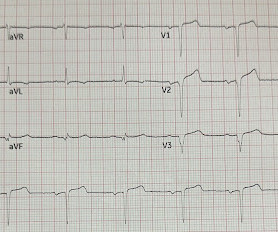
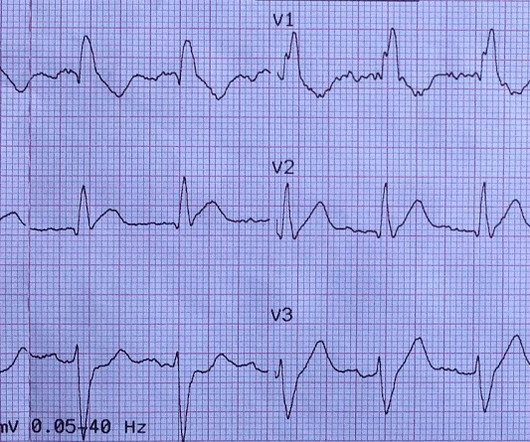
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" She had a proven 100% Left Main occlusion No ST shift in aVR This pattern of RBBB/LAFB was also the most common pattern in Fiol et al.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. References: Jaff MR et al. PMID: 21422387 Wan S et al. PMID: 15262836 Sharifi M et al. PMID: 27422214 Wang C et al. PMID: 19741062 Kucher N et al. PMID: 24226805 Piazza G et al. Clin Exp Emerg Med 2023. CHEST 2010.
It is reasonable to administer vasodilators (eg, nitrates, phentolamine, calcium channel blockers) for patients with cocaine-induced coronary vasospasm or hypertensive emergencies. Editorial Comment : Use standard BLS/ALS measures, especially if in cardiac arrest. COR 2a, LOE C-LD. COR 2a, LOE C-LD. COR 1, LOE C-LD. COR 1, LOE C-EO.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiac arrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. Finally, head-up CPR (which was not used here), makes for better resuscitation.
See this paper by Widimsky et al, which shows the high association of RBBB, especially with LAFB, with LAD occlusion. Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAH) on the admission ECG. New RBBB + LAFB is a very bad sign.
Clinical Question : In patients who suffer an OHCA without ST-segment elevation on the post-resuscitation ECG, will early coronary angiogram (CAG) vs. delayed CAG improve outcomes? Article: How-Berlemont C, Lamhaut L, Diehl J, et al. Early coronary angiography and survival after out-of-hospital cardiac arrest. Nallamothu, B.
It was witnessed, and CPR was performed by trained individuals. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. Updates on the Electrocardiogram in Acute Coronary Syndromes. Electrocardiogram patterns in acute left main coronary artery occlusion. see below). References : 1. Nikus KC, Eskola MJ.
1 The primary goal of cardiopulmonary resuscitation (CPR) is to optimize coronary perfusion pressure and maintain systemic perfusion in order to prevent neurologic and other end-organ damage while working to achieve ROSC. Nielsen N, Wetterslev J, Cronberg T et al. By the time of the study by Nielsen et al. New Engl J Med.
Medics found her apneic and pulseless, began CPR, and she was found to be in asystole. Rather it is due to coronary insufficiency due to a tight left main or 3-vessel disease with inadequate coronary flow. Kurkciyan et al. Kurkciyan et al., A middle-age woman with h/o hypertension was found down by her husband.
He underwent CPR, and regained a pulse after epinephrine, with an organized narrow complex rhythm at 140, but still with severe shock. And so it is wise to look at the coronary arteries. This ECG certainly looks like myocarditis, and was due to myocarditis, but missing acute coronary occlusion is not acceptable. 3–8 Shi et al.
Is there likely to be fixed coronary stenosis that led to demand ischemia during pneumonia? --Was See this paper by Widimsky et al, which shows the high association of RBBB, especially with LAFB, with LAD occlusion. 30 minutes later, this ECG was recorded: There is less high lateral ST elevation And another 3.5
Data that do not establish neurological risk stratification in the first 6 hours after CA include the patient’s age, duration of CPR, seizure activity, serum lactate level or pH, Glasgow motor subscore in patients who received NMB or sedation, pupillary function in patients who received atropine, and optic nerve sheath diameter (95.3%, 20/21).
Raitt MH, et al. Methods: Oliva et al. (94) Patients who received CPR or experienced reinfarction or very small infarcts due to thrombolysis also displayed Type II T-wave evolution. Methods: Oliva et al. Mauri F, Gasparini M, Barbonaglia L, et al. Am J Cardiol 1989; 63:1291-1295 Methods: Mauri et al.
Paper 1: Schmidt HJ et al. PMID: 360027567 [ Access on Read by QxMD ] Paper 2: Kjaergaard J et al. References: Schmidt HJ et al. PMID: 360027567 [ Access on Read by QxMD ] Kjaergaard J et al. A higher MAP may offer advantages due to improved cerebral perfusion pressure, however data is lacking. Liberal O2: 33.9%
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chest pain and collapsed, and had bystander CPR. This ALONE is very strong evidence of acute coronary occlusion. Any indications for cath lab activation?
the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. We could not resuscitate her, but we did have excellent perfusion with LUCAS CPR, such that pulse oximetry had excellent waveform and 100% saturations, end tidal CO2 was 35, and cerebral perfusion monitoring was near normal throughout the attempted resuscitation.
Nizami T, Beaudoin F, Suner S, et al. Reviewed by: Vicki Currie Article 5: Does occluding the femoral artery during neonatal CPR increase the likelihood of ROSC? (In Both were partly delivered via caesarian section, flow probes inserted into carotid, pulmonary and left circumflex coronary arteries. Crocker, B.C.S.,
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content