This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. The proof of this is that only 5% of patients enrolled had acute coronary occlusion. Lemkes JS, Janssens GN, van der Hoeven NW, et al. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. 5% vs. 58%!!
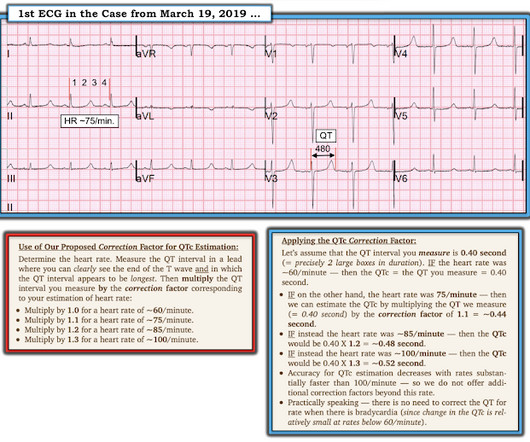
Bogossian et al. (1) Bogossian H, Frommeyer G, Ninios I, Hasan F, Nguyen QS, Karosiene Z, Mijic D, Kloppe A, Suleiman H, Bandorski D, et al. Among patients with left bundle branch block, T-wave peak to T-wave end time is prolonged in the presence of acute coronary occlusion. Then we can correct that modified QT for heart rate.
2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. Initial guidelines defined “refractory” as VT or VF occurring despite three shocks from a cardiac defibrillator. Tips for use of dual sequence defibrillation 11 : Use the same model of defibrillator.
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients.
Article: Branch KHR et al. Indication for emergency invasive coronary angiography or had coronary angiography within 1 hour of arrival. Known obstructive coronary artery disease or known coronary stent. Known cardiac defibrillator. References: Branch KHR et al. Resus 2023. Pre-existing DNR order.
It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). Upon contrast injection of the LMCA, the patient deteriorated, as the LMCA was severely diseased and flow to all coronary arteries ( LAD, LCx and RCA ) was compromised. He was taken immediately to the cath lab.
We can, therefore, put down the defibrillation pads, set aside the amiodarone, and look further at the ECG. The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Paradoxically, though, the third green arrow identifies a QRS that is more narrow than the RBBB complexes surrounding it. References Chiale, P.
Below is the version standardized by PM Cardio app Meyers interpretation: Findings are specific for posterior (and also likely inferior) wall transmural acute infarction, most likely due to acute coronary occlusion (OMI). Most OMI have a peak Troponin T over 1000 ng/L [reference: Baro R et al. Clinical Cardiology 2019.
He underwent further standard resuscitation EXCEPT that we applied the Inspiratory Threshold Device ( ResQPod ) AND applied Dual Sequential Defibrillation (this simply means we applied 2 sets of pads, had 2 defib machines, and defibrillated with both with only a fraction of one second separating each defibrillation.
He underwent coronary angiography which showed severe multivessel disease, and he agreed to proceed with workup for CABG. But artifact is "alive and well" — and learning to recognize it will amaze many of your colleagues ( and may serve to avoid an unnecessary defibrillation or two ). I immediately thought this tracing looked bizarre!
Even though the primary suspicion was not ischemic heart disease, a CT angiogram was performed, and it revealed normal coronary arteries. This ruled out coronary disease as the cause of conduction system disease. She was given CRT-D (Cardiac Resynchronization Therapy-Defibrillator).
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She was immediately intubated during continued compressions, then underwent a 9th defibrillation, which resulted in an organized rhythm at 42 minutes after initial arrest. see below).
She was defibrillated and resuscitated. Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al.
After resuscitation and defibrillation , there were no more episodes of TdP. A coronary angiogram was done that did not show significant coronary artery disease. A coronary angiogram was done that did not show significant coronary artery disease. Below is the patient’s 12 lead ECG following defibrillation.
Armstrong et al. The patient has also developed sinus bradycardia, which may result from right coronary artery ischemia to the SA node. During angiogram in the cath lab, the patient suffered two episodes of ventricular fibrillation for which he was successfully defibrillated. Two stents were placed with resultant TIMI 3 flow.
She was never seen to be in ventricular fibrillation and was never defibrillated. Rather it is due to coronary insufficiency due to a tight left main or 3-vessel disease with inadequate coronary flow. Kurkciyan et al. Kurkciyan et al., With ventilations and epinephrine, she regained a pulse. BP gradually rose.
Meyers et al. Accuracy of OMI findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardial infarction. Aslanger et al. DIagnostic accuracy oF electrocardiogram for acute coronary OCClusion resulTing in myocardial infarction (DIFOCCULT study). Lemkes et al. Bergmark et al.
This page summarises the most current recommendations for the management of acute coronary syndromes with persistent ST-segment elevations (i.e This page summarises the most current recommendations for the management of acute coronary syndromes with persistent ST-segment elevations (i.e
At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. He was given amiodarone and lidocaine load and drip and K and Mg drips. 1987;147(3):465-469.
Written by Willy Frick with edits by Ken Grauer An older man with a history of non-ischemic HFrEF s/p CRT and mild coronary artery disease presented with chest pain. The most common way is by delivering a lead into the coronary sinus ostium in the RA, which wraps around the posterolateral portion of the LV. Kaye et al.
ONLY give opiates if the pain is intolerable or you will activate the cath lab at the first objective evidence of coronary ischemia. In this case, you should get a second defibrillator and perform double sequential external defibrillation (DSED). The patient was taken to lab for coronary angiography.
Moreover, it does not follow a coronary distribution very well. The coronaries were clean. By ECG alone: it is suspicious for stress cardiomyopathy, or takotsubo, due to the diffuse ST Elevation: II, III, aVF AND I and aVL. This is unusual in acute OMI. In addition, there is STE in V3-V6, so there is massive injury. From this site.
CT coronary angiogram showed a hypoplastic RCA and dominant LCx. Most patients can be managed without and implantable cardioverter defibrillator (ICD) In patients with PVCs/VT and a presentation not typical for an idiopathic origin cardiac magnetic resonance (CMR) should be considered, even if the Echo is normal. . No PVCs are seen.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content