This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. We documented that the majority of stenotic lesions had compensatory enlargement and thus exhibited remodeling.
An unknown EP reviews the report, determines that there is no reason to notify the patient, and documents nothing. Autopsy shows coronary atherosclerosis and marked cardiomegaly with a thickened left ventricular wall. It wasn’t, so you weren’t called, nor did the doc need to document anything. Baccei SJ et al.
In fact, Kosuge et al. showed that among patients with either acute coronary syndrome or acute pulmonary embolism and negative T waves in the precordial leads (V1-V4), that inverted T waves in leads III and V1 were present in only 1% of patients with acute coronary syndrome and 88% of patients with pulmonary embolism. “The
It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). Upon contrast injection of the LMCA, the patient deteriorated, as the LMCA was severely diseased and flow to all coronary arteries ( LAD, LCx and RCA ) was compromised. He was taken immediately to the cath lab.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. References: Jaff MR et al. PMID: 21422387 Wan S et al. PMID: 15262836 Sharifi M et al. PMID: 27422214 Wang C et al. PMID: 19741062 Kucher N et al. PMID: 24226805 Piazza G et al. Clin Exp Emerg Med 2023. CHEST 2010.
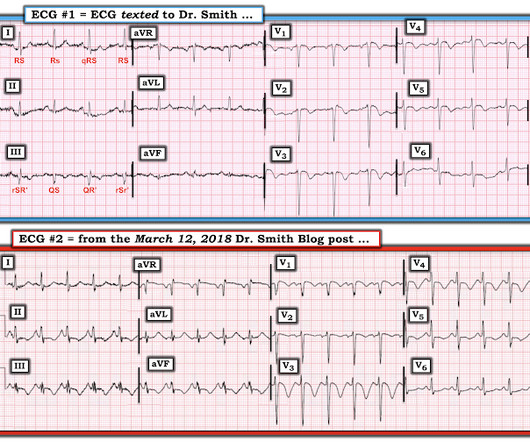
The documentation does not describe any additional details of the history. They also documented "Reproducible chest tenderness." Heitner et al. We know that even high-sensitivity troponin may not exceed the "normal" range for a period of hours in certain patients with acute coronary occlusion. ECG 1 What do you think?
He had no previously documented medical problems except polysubstance use. Serial ECGs enhance the diagnosis of acute coronary syndrome. Bigger et al. Association of intravenous morphine use and outcomes in acute coronary syndromes: Results from the Crusade Quality Improvement Initiative. Leave it alone.
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present."
It is well documented with continuous 12-lead monitoring that acute re-occlusion is frequently asymptomatic. It shows that on a 7 day angiogram, only 58% of re-occlusions were symptomatic: Ohman EM, Califf RM, Topol EJ et al. Akkerhuis KM, et al. Gottlieb SO, et al. Jernberg T, et al. Patel DJ, et al.
Background: Historically, we have treated acute coronary syndrome with supplemental oxygen regardless of the patient ’ s oxygen saturation. More recent evidence, however, demonstrates that too much oxygen could be harmful ( AVOID Trial ) by causing coronary vasoconstriction and increasing oxidative stress. Low O2 protocol: 3.1%
Dr. Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al. Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al.
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. References Hansen MS, et al. Rogers AM, et al. Cecconi M, et al. Then what?
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published. P.S.: Our September 3, 2020 post features Dr.
STEMI criteria is bad at differentiating between normal variant and acute coronary occlusion or reperfusion, and initial troponin levels don't differentiate between occlusive and non-occlusive MI 3. the presence of J waves from early repolarization doesn’t rule out an acute coronary occlusion 4. McLaren et al, including Meyers/Smith.
I was not worried for a coronary etiology. PEARL #3: The pathophysiologic mechanism for producing amphetamine-induced acute MI is unclear ( Bazmi et al — SQUMJ 17(10); e31-37, 2017 — and — Sinha et al — Case Rep Cardiol, 2016 ). The precordial findings are typical for a young AA male See 20 similar cases here.
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. The condition of the coronary artery at the time of angiogram may be different than it was 30 minutes prior during recording of the ECG. A 40-something woman had sudden chest pain. She called 911. The proposed mechanism is complex.
The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. Our patient had a Brugada Type 1 pattern elicited by an elevated core temperature, which is also a documented phenomenon. In the largest study looking at this topic by Mizusawa et al.,
Early coronary angiography in post-CA patients with no ST-segment elevation on the presenting ECG may still be of benefit by potentially salvaging myocardium and decreasing the incidence of systolic heart failure in survivors (95.7%, 22/23). Individualize RBCTs to the clinical situation (81%, 17/21).
Tintinalli JE, Stapczynski J, Ma O, et al. Acute myocardial infarction with normal and near normal coronary arteries. Documentation with coronary arteriography within 12 1/2 hours of the onset of symptoms in two cases (three episodes). Arnoldo BD, Purdue GF, Kowalske K, et al. 2023 Jul 17. McGraw Hill; 2016.
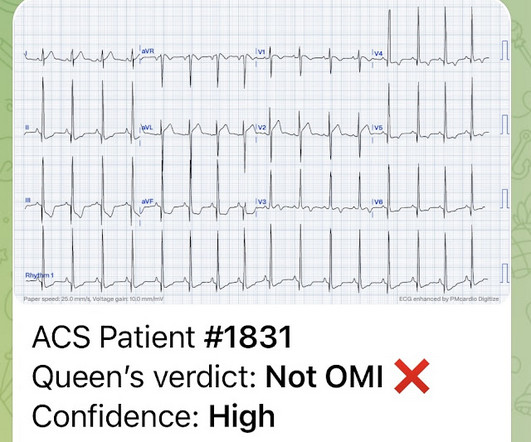
His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." Chest pain is documented as ongoing. NOTE: For illustrative purposes — I’ve adapted Figure-1 from the original manuscript by deWinter et al, published in this 2008 NEJM citation. QOH: "OMI High confidence".
The patient was in his 50s with history of hypertension, diabetes, seizure disorder, and smoking, but no known coronary artery disease. No patient should have to be "lucky" by having a positive troponin to be taken seriously as a possible acute coronary occlusion. See the proof for yourself in the literature below: Schmitt et al.
Article: Kumar M et al. References De Pietri L, Bianchini M, Montalti R, et al. PMID: 31229583 Kumar M, Ahmad J, Maiwall R, et al. PMID: 31148204 Rout G, Shalimar, Gunjan D, et al. PMID: 20335313 Wang SC, Shieh JF, Chang KY, et al. Hepatology. 2020;71(1):235-246. Significant coagulopathy: INR > 1.8
Kosuge et al. Witting et al. This does not contradict the conclusions of Kosuge et al. , Finally, Stein et al. This is a paper worth reading : Marchik et al. Finally — Note that the S1Q3T3 pattern is missing in ECG #2 , despite documentation of a massive PE. of controls.
This page summarises the most current recommendations for the management of acute coronary syndromes with persistent ST-segment elevations (i.e III A Primary percutaneous coronary intervention strategy Management Recommendation Level of evidence Primary PCI of the infarct related artery (IRA) is indicated.
Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia." the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. Over a 13-month period, serum potassium and magnesium levels were measured in 590 patients admitted to a coronary care unit. 1987;147(3):465-469.
According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. Cardiology documented “late presentation STEMI but likely aborted given resolution of ST changes from EMS to hospital.”
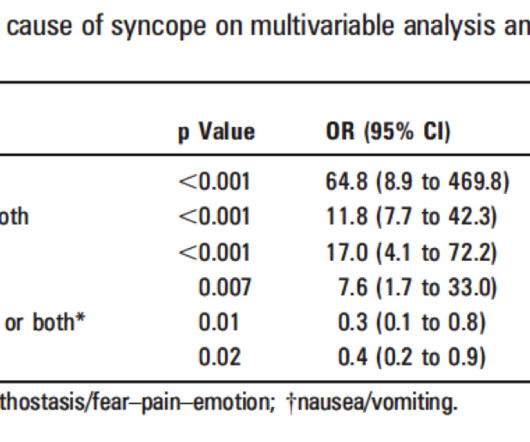
Also consider non-hemorrhagic volume depletion, dehydration : orthostatic vitals may uncover this [see Mendu et al. (3)]. Thus, if there is documented sinus bradycardia, and no suspicion of high grade AV block, at the time of the syncope, this is very useful. Del Rosso A, et al. Other studies 1) EGSYS score (full text link).
There is very scarce documentation, but the next ECG was obtained around 1 PM. A recent meta-analysis by Stone et al. In fact, this incredible study by Heiter et al. There was no repeat ECG. There was repeat troponin about an hour after that, and it trended down, from 41 ng/L to 30 ng/L, now within the reference range.
ONLY give opiates if the pain is intolerable or you will activate the cath lab at the first objective evidence of coronary ischemia. Documentation indicates that the patient was shocked 4 times (with no comment on energy level) and received amiodarone 300 mg IV and magnesium 2 g IV. In fact, in this elegant study by Heitner et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content