This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The 2022 American College of Cardiology (ACC) pathway provides timely guidance [1]. Intermediate-risk patients may be further stratified based on recent stress testing or coronary angiogram findings plus a modified HEART or Emergency Department Assessment of Chest Pain (EDACS) score. Time to know your hs-cTn better.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Challenge QUESTION: The relative change in T-QRS-D is not the only thing that changes during period of time that passed between recording of the 2 ECGs shown in Figure-1.
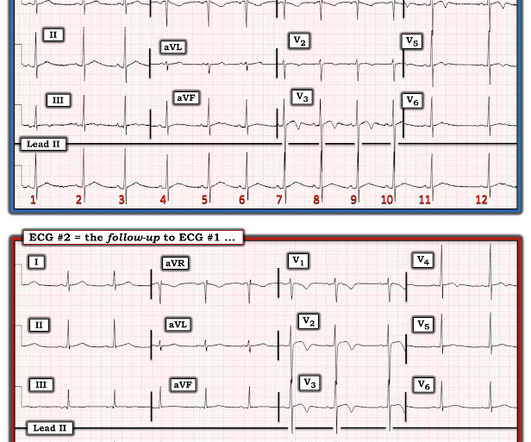
Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Here is lead I from ECGs 1 and 2 shown side-by-side to highlight the change in axis from borderline right to completely normal. While not completely ruling out acute coronary disease — another cause should be considered.
Coronaries were clean. I agree, however: 1) I don't think you can get a good enough ech o without bubble contrast. 3) E cho is another step that takes time. I agree, however: 1) I don't think you can get a good enough ech o without bubble contrast. 3) E cho is another step that takes time. Time is myocardium.
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. C Examination notable for diaphoresis, 1+ bilateral lower extremity edema, regular heart rate and rhythm, and no signs of respiratory distress with normal breath sounds. In fact, Kosuge et al. Stein et al. Kosuge et al.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chest pain onset around 9 PM the evening prior. ECG 1 What do you think? Grines, C.
Initial vital signs include: NIBP 99/58 HR 150-160 (trend) RR 10 (spontaneous, but shallow) SpO2 86 (RA) BBS CTA The initial rhythm strip is attached: Figure 1 There is a wide complex tachycardia of varying morphology, amplitude, and R-R cycle length. A prominent vertical scar, however, is noted at the sternum.
Question 1: What is the rhythm? Beat 1 : Sinus, narrow QRS complex. The assumption is that a premature complex discharged prior to Beat 1, which prolonged its respective refractory period in the same manner as Beat 5. The coronary angiogram revealed no critical stenosis, or acute plaque ulceration.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. So maybe she is better than I am.
1 The shortage in supply posed difficulties for hospitals that significantly depend on GE Healthcare as their supplier, which encompassed approximately 50% of hospitals in the United States (US). 11 Table 1. Preparation 9 Hospitals had to prepare for the impending contrast shortage as soon as potential shortage news occurred.
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiac arrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. Figure-1: The initial ECG in today's case — obtained after ROSC.
The data in the paper by Rangel et al. Vittinghoff, E. Metoprolol and atenolol are overwhelmingly beta-1 cardioselective. Beta-1 blockade decreases inotropy and chronotropy and has no vasoconstrictive effects. is intuitive, and not surprising. style='mso-element:field-begin'> ADDIN EN.CITE Rangel 1853 1853 17 Rangel, C.
Learning Points: 1. If the situation is not right for acute coronary occlusion, then the ECG findings probably do not represent acute coronary occlusion. Despite the eye-catching ST-T wave changes that came-and-went a number of times — there was no acute coronary occlusion. Figure-1: The first 2 tracings in today's case.
Most agents exhibit both vasopressor and inotropic effects (Figure 1). Below follows a drug manual for use in the CCU (coronary care unit), ICU (intensive care unit) or ER (emergency room). μg/kg/min + + + ++ Low dose dopamine stimulates D1 receptors and induces vasodilation in coronary, renal, cerebral and mesenteric vessels.
mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. What do you think?
And so it is wise to look at the coronary arteries. Here they are: Learning Points: 1. This ECG certainly looks like myocarditis, and was due to myocarditis, but missing acute coronary occlusion is not acceptable. 3–8 Shi et al. In acute MI, the T-wave is large, and the T/ST ratio is high. Angiogram was negative.
But these cases show the potential dangers of delayed recognition and treatment of inferior reperfusion Take away 1. ECG’s can be labeled as ‘normal’ by the computer (and confirmed by cardiology) even with diagnostic signs of occlusion or reperfusion References 1. Backus BE, Six AJ, Kelder JC, et al. JAMA Intern Med 2019 9.
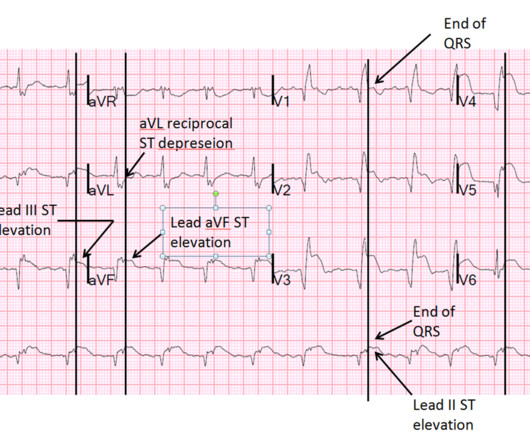
There are two main etiologies of ischemic ST-depression: 1) subendocardial ischemia 2) reciprocal to ST-elevation in an opposite wall Here there are distinct R-waves with marked ST-depression throughout most of the precordium. Tips for recognizing Acute Posterior STEMI: 1. References: 1. O'Gara et al.
Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Raitt et al.) [and Armstrong et al.)], the presence of such well developed anterior Q-wave suggests completed transmural STEMI. 3) Oliva et al. (3) Armstrong PW et al. J Am Coll Cardiol 53(17):1503-9. Very unlikely.
4 important features that indicate acute right hear strain: 1. Kosuge et al. In this study, (quote) "negative T waves in leads III and V 1 were observed in only 1% of patients with ACS compared with 88% of patients with APE (p less than 0.001). Witting et al. Finally, Stein et al. Tachycardia (or nearly) 2.
Article: Kumar M et al. 2020;71(1):235-246. Plt 37×10^9/L and 40×10^9/L, SOC and TEG, respectively) All patients enrolled had an upper endoscopy and verified the source of bleeding. Hepatology. Significant coagulopathy: INR > 1.8 Significant coagulopathy: INR > 1.8
He had episodes of chest pain off and on all night, until about 1 hour prior to arrival when the pain became constant, crushing, 10/10 chest pain that radiated to both arms. Proven STEMI has an open artery in 19% to 36% of cases, depending on whether it is TIMI −1, −2, or −3 flow. 25] Stone et al found that 72% have TIMI 0 or 1 flow.
Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Raitt et al.), Armstrong et al.), 3) Oliva et al. (4) He found 2 ECG patterns of atypical T-wave development in PIRP: 1) persistently positive (upright) T-waves 48 hours after AMI onset. Lessons : 1. Armstrong PW et al.
1 The primary goal of cardiopulmonary resuscitation (CPR) is to optimize coronary perfusion pressure and maintain systemic perfusion in order to prevent neurologic and other end-organ damage while working to achieve ROSC. Nielsen N, Wetterslev J, Cronberg T et al. By the time of the study by Nielsen et al. 2019;23(1):1–9.
Ct coronary angiogram showed normal coronary arteries. Smith note: I think CT coronary angiogram is reasonable with the elevated troponins and symptoms. The Cardiorespiratory Implications of Ultra-marathon Bjørkavoll‐Bergseth et al. Paana et al. He was diagnosed with mild AKI which resolved. ng/L; 3 hours, 38.3
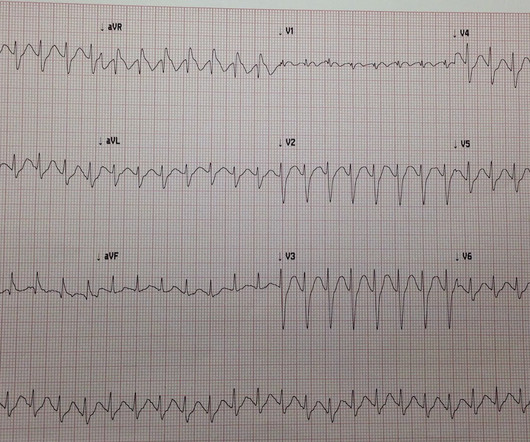
A 40-something male presented with dyspnea and left arm numbness, and perhaps some chest tightness, for 11/2 hours. Thelin et al. Mokhtari et al. E CG # 1 = the initial Triage ECG ( TOP ) — As per Dr. . = Here is his triage ECG: There is massive STE in V3-V6, and also STE in II, III, aVF.
The neurologic section was divided into (1) brain oxygenation, perfusion, edema, and intracranial pressure (ICP); (2) seizures and the ictal-interictal continuum (IIC); and (3) sedation and analgesia. Reference: Hirsch KG, Abella BS, Amorim E, et al; American Heart Association, Neurocritical Care Society. 2023 Dec 1.
The Differential Diagnosis is: SVT with aberrancy(#) [AVNRT vs. WPW (also called AVRT*)] Atrial flutter with 1:1 conduction, with aberrancy VT coming from the anterior fascicle ( fascicular VT )@ *AVRT = AV Reciprocating Tachycardia (Tachycardic loop that uses both the AV node and an accessory pathway. See Learning point 1 below.
1 week later (about 1 week prior to the tamponade visit) she had a follow up outpatient visit and this ECG was recorded: Appears to show resolving findings. For an excellent review of the pathophysiological explanation of signs and symptoms associated with Pericardial Tamponade SEE this Review by Jensen et al in the e-Journal Card.
1 Indications for transplant include: Non-ischemic cardiomyopathy (49%) Ischemic cardiomyopathy (35%) Restrictive cardiomyopathy (4%) Retransplantation following failed prior transplant (3%) Hypertrophic cardiomyopathy (3%) Congenital heart disease (3%) Valvular cardiomyopathy (3%) The median survival after heart transplant is over 12 years.
1 One study found that CTA head and neck was ordered for 2.5% 2 Outcomes of patients presenting with ischemic stroke who received MRI as initial imaging modality have demonstrated similar outcomes to those with initial CTA, with Kim et al. In a study of 17,903 CTAs ordered in the ED, Tu et al. 8 The data in Mayer et al.
1 The ED is a fast-paced environment where patient stability and life-and-limb-threatening conditions are prioritized. The pain began abruptly 1 hour ago, described as a stabbing sensation, and has occurred daily at the same time for the past week, each episode lasting about 45 minutes. Pain can be improved or exacerbated with meals.
She describes the pain as left-sided, non-radiating, and 9/10 in severity. The catheterization lab is activated, but catheterization shows no coronary artery occlusion. A 67-year-old female with past medical history of hypertension presents with acute onset of chest pain without associated symptoms. What is the diagnosis?
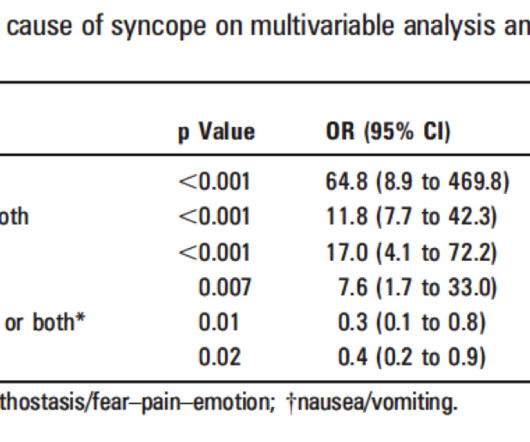
Also consider non-hemorrhagic volume depletion, dehydration : orthostatic vitals may uncover this [see Mendu et al. (3)]. Cardiac Syncope ("True Syncope") Independent Predictors of Adverse Outcomes condensed from multiple studies 1. Palpitations preceding syncope (highest value on EGSYS score) 9. S yncope while supine (EGSYS) 8.
Chu CK, Delia E, Mograder A, Dwyer EM. 2017;45(1):12-20. 2017;45(1):12-20. doi:10.1016/S0033-0620(05)80036-2 Balik M, Novotny A, Suk D, et al. 2015;7(9):E365-E369. doi:10.3390/JCM13185344 Yamagishi T, Tanabe T, Fujita H, et al. 2018;12(1). J Saudi Hear Assoc. 2018;30(4):336. doi:10.1016/J.JSHA.2018.07.001
Moreover, it does not follow a coronary distribution very well. The coronaries were clean. Today's patient unfortunately developed PEA ( P ulseless E lectrical A ctivity ) arrest shortly after arrival of the medic team. This is unusual in acute OMI. In addition, there is STE in V3-V6, so there is massive injury. From this site.
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. The scan showed a bicuspid aortic valve with severe stenosis and coronary artery disease. The top ECG is diagnostic of thrombotic type 1 OMI until proven otherwise.
Although these autoantibodies may be present in a variety of individuals, the development of clinical disease is thought to require exposure to an environmental risk factor such as certain viruses, cigarette smoke or other environmental toxins (1). million have been diagnosed with lupus, with 90% of cases occurring in females (1).
This is likely because Dexmed helps dampen the sympathetic response to perioperative stress, improving coronary artery perfusion. While no paediatric studies have confirmed this, the DICE trial ( D exmedetomidine in I nfants undergoing C ooling for Neonatal E ncephalopathy) is underway. 2021.770511 Bayram A, Ulgey A, Baykan A, et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content