This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
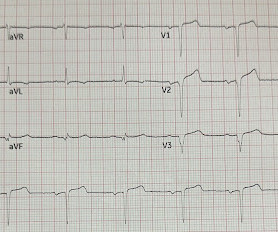
Date: November 22, 2023 Reference: Stopyra et al. Date: November 22, 2023 Reference: Stopyra et al. A 12-lead electrocardiogram (ECG) demonstrates ST elevations in leads II, III, and aVF with ST depressions in leads I and aVL and the team begins transport to the nearest percutaneous coronary intervention (PCI) capable hospital.
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Detailed coronary artery evaluation not performed.
Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? AEM June 2022. AEM June 2022.
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP).
Additional architectural changes include systolic anterior motion of the mitral valve, endothelial dysfunction at the level of the coronary arterial bed, and ventricular diastolic dysfunction. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. Below is the initial ED ECG.
Date: January 16th, 2020 Reference: Troponin Testing and Coronary Syndrome in Geriatric Patients With Nonspecific Complaints: Are We Overtesting? Date: January 16th, 2020 Reference: Troponin Testing and Coronary Syndrome in Geriatric Patients With Nonspecific Complaints: Are We Overtesting? Reference: Wang et al.
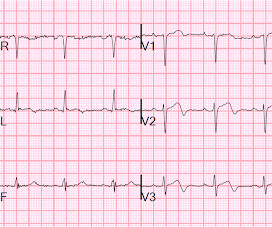
One cannot rely on this feature as a means of detecting changes – subtle, or dramatic – for volatile occlusive coronary thrombus. Here is the final ECG just prior to ED transfer. Attached below is the initial ED tracing upon hospital arrival, approximately 25 minutes after the prehospital ECG. No serial ECG’s were recorded.
emergency departments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. References Tsao CW, et al. Benjamin EJ, et al. Kimblad H, et al. Sakai T, et al. Kudenchuk PJ, et al. Lee YH, et al. Benjamin EJ, et al. Hajjar K, et al. Circulation.
It was present on arrival at triage but then resolved before bed placement in the ED. This is a demonstration of how Wellens' is transient OMI : First ED ECG is Wellens' (pain free). Lemkes JS, et al. It is a ssociated with mild dyspnea on exertion. At times the pain does go to his left neck. Am Heart J. 2000;139:430–436.
The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Takotsubo should be a diagnosis of exclusion after angiography reveals no obstructive coronary disease, and repeat Echo displays left ventricular recovery. Chou’s Electrocardiography in Clinical Practice (6th ed). References Chiale, P. Saini, A.,
The latest is Langlois-Carbonneau et al. Our data corroborate that immediate management of a patient with a normal automated triage ECG reading is not modified by real-time ED physician ECG interpretation." But according to Langlois-Carbonneau et al., Safety and accuracy of the computer interpretation of normal ECGs at triage.
Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ).
Date: May 24th, 2022 Reference: Broder et al. Date: May 24th, 2022 Reference: Broder et al. The writing group of GRACE-2 wanted to look at clinically relevant questions to address the care of adult patients with low-risk, recurrent, previously undifferentiated abdominal pain in the ED. Reference: Broder et al.
Coronaries were clean. Not OMI with High Confidence Click here to sign up for Queen of Hearts Access We showed that the Queen of Hearts decreases false positive cath lab activations: 1) Published recently in Prehospital Emergency Care Baker PO et al. 2) To be presented at AHA conference in Chicago in 2 weeks: Sharkey SW et al.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). link] [1] Zachary et al. Utility of the history and physical examination in the detection of Acute Coronary Syndromes in emergency department patients. Chou's Electrocardiography in Clinical Practice, 6th ed.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So the patient had a transient acute coronary occlusion that spontaneously reperfused but is at risk for reocclusion. Deutch et al.
A 3-year-old male with no past medical history presents to the ED with one week of daily fevers >102°F associated with four days of rash on the trunk. We’ll keep it short, while you keep that EM brain sharp. Tomisaku Kawasaki, who noticed 50+ similar pediatric presentations between the years 1961 and 1967. C) for the past week.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
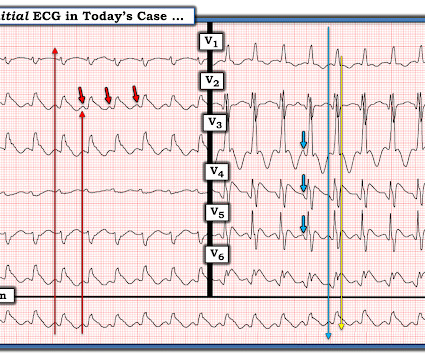
Below is the version standardized by PM Cardio app Meyers interpretation: Findings are specific for posterior (and also likely inferior) wall transmural acute infarction, most likely due to acute coronary occlusion (OMI). Most OMI have a peak Troponin T over 1000 ng/L [reference: Baro R et al. Clinical Cardiology 2019.
When the patient arrived in the ED, he was still hypotensive in 70s, slowly improving with EMS fluids. Here is the ED ECG (a photo of the paper printout) What do you think? QOH ( Q ueen O f H earts ) and Dr. Smith's former resident immediately diagnosed acute OMI — but providers in the ED thought the ECG findings "looked old".
He arrived in the ED and had this ECG recorded: There are Wellens' waves, type A (upsloping ST segment then inversion of the terminal part of the T-wave - terminal T-wave inversion, or biphasic T-waves) in V2-V4, and aVL. This male in his 40's had been having intermittent chest pain for one week. de Zwaan C., Janssen J.H.A., de Zwaan C.,
Here is his initial ED ECG: What do you think? Then the ED doc would be dependent on that first ECG. It must have re-occluded between the ED and the cath lab) --Lesion was stented. Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.) have perfect coronary flow by the time of angiogram.
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present."
” – Musings of an American ED resident in July 2022 when US healthcare was affected simultaneously by supply chain issues from GE Healthcare (contrast media) and Abbott Laboratories (Similac baby formula). 3 A study of CT use trends in the ED has shown increasing use of CTs by almost 60% from 2005 to 2013.
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. Chou’s Electrocardiography in Clinical Practice, 6th ed. 4] Baranchuk, A, et al. Goldberger’s Clinical Electrocardiography: A Simplified Approach, 9th ed.
But the paramedic and the ED physician in this case did not subscribe to this idea. I have here 38 cases of "Computer Normal" ECGs which were critically abnormal and the vast majority are missed acute coronary occlusions (Missed Acute OMI) and most were recognized by the physician. So this study is worthless and must be ignored.
Dr. Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al. Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al.
Video 3: Coronary approach to the gallbladder POCUS Findings Sonographically, the gallbladder is situated in the right upper quadrant as an elongated pear-shaped organ on the inferior surface of the liver. Ross M, Brown M, McLaughlin K, et al. Dumbrava BD, Bass GA, Jumean A, et al. Al-Khouja F, Mazumder P, Moeller J, Lahham S.
This post will focus on the key parts of the guideline that affect ED evaluation and management. It is reasonable to administer vasodilators (eg, nitrates, phentolamine, calcium channel blockers) for patients with cocaine-induced coronary vasospasm or hypertensive emergencies. Top 10 Take Home Pearls 1. COR 2a, LOE C-LD.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago.
They arrived in the ED 30 minutes later to meet the cardiology team, where an ECG was repeated: Again no STEMI criteria, and there has been improvement in the deWinter and swirl pattern. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
It was worse on the evening prior to presentation while lying in bed, then recurred and resolved while at rest just prior to arriving in the ED. Here is the first ED ECG, with no pain: Sinus rhythm. It shows that on a 7 day angiogram, only 58% of re-occlusions were symptomatic: Ohman EM, Califf RM, Topol EJ et al. de Wood et al.
link] A 30 year-old woman was brought to the ED with chest pain. The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This is written by Brooks Walsh.
A 68-year-old male with a past medical history of hypertension, diabetes mellitus, and coronary artery disease with a drug eluting stent placed 2 months ago presents with dizziness and vomiting that began 3 hours ago. Median time from ED arrival to diagnosis was 8 hours 24 min in one study, with only 19% being diagnosed within the 4.5-hour
Written by Jesse McLaren Two patients in their 70s presented to the ED with chest pain and RBBB. The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. Coronaries were normal, as was serial troponin. Vitals were normal.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The De Winter ECG pattern: morphology and accuracy for diagnosing acute coronary occlusion: systematic review. 2009;95:1701–1706.
The patient arrived in the ED and had this ECG: No difference. All coronaries were completely normal. Only 5-13% of patients with chest pain and LBBB have MI; many fewer have coronary occlusion. Additionally, appropriate discordance is common in NonSTEMI, but very unusual in coronary occlusion (STEMI).
Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. It can only be seen by IVUS. MINOCA has many etiologies.
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery disease? Knotts et al. Left main?
Here is the ED ECG on arrival: Less STE/STD Provider's Clinical Impression: "findings concerning for myocardial infarction, likely proximal LAD or Left main." The case I presented in My Comment to that March 9, 2020 post showed a patient with this pattern — who on cath had no more than minimal coronary disease.
ECG 1 at time zero EARLY REPOLARIZATION ABNORMAL ECG ED final official overread: "early repol vs hyperacute T, minimal changes from previous (previous shown below)" What do YOU think? Lemkes et al. See these casese (and I have many others): First ED ECG is Wellens' (pain free). A 70-something y.o. Eur Heart J 2018. Am Heart J.
I want all to know that, with the right mind preparation, and the use of the early repol/LAD occlusion formula, extremely subtle coronary occlusion can be detected prospectively, with no other information than the ECG. This was my thought: if this patient presented to the ED with chest pain, then this is an LAD occlusion. Asymmetric.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















































Let's personalize your content