This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
On a busy day shift in the emergencydepartment, our seasoned triage nurse comes to me after I finish caring for a hallway patient, “Hey, can you come see this guy in the triage room? This is the essence of emergency medicine. Knack SKS, Scott N, Driver BE, Pet al. Ann Emerg Med. His vitals are fine…”.
Intermediate-risk patients may be further stratified based on recent stress testing or coronary angiogram findings plus a modified HEART or EmergencyDepartment Assessment of Chest Pain (EDACS) score. The patient has no previous stress testing or coronary angiogram, and he is not low risk by HEART or EDACS scoring.
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
Date: September 23, 2024 Reference: Essat et al. Annals of Emergency Medicine, May 2024 Guest Skeptic: Dr. Casey Parker is a Rural Generalist from Australia who is also an ultrasounder. The patient has no specific risk factors for acute coronary syndrome (ACS) or dissection. Reference: Essat et al.
[display_podcast] Date: October 17th , 2018 Reference #1: Aycock, Westafer et al. Ann Emerg Med 2018 (CRD42017056195) Reference #2: Weisbord SD, Gallagher M, Jneid H, et al; PRESERVE Trial Group. first appeared on The Skeptics Guide to Emergency Medicine. Reference: Aycock, Westafer et al.
Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Guest Skeptic: Dr. Corey Heitz is an emergency physician in Roanoke, Virginia. He is also the CME editor for Academic Emergency Medicine. Reference: McGinnis et al.
Date: September 8th, 2021 Reference: Desch et al. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. first appeared on The Skeptics Guide to Emergency Medicine. Date: September 8th, 2021 Reference: Desch et al.
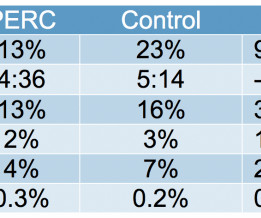
[display_podcast] Date: May 16, 2018 Reference: Freund et al. Effect of the Pulmonary Embolism Rule-Out Criteria on Subsequent Thromboembolic Events Among Low-Risk EmergencyDepartment Patients: The PROPER Randomized Clinical Trial. display_podcast] Date: May 16, 2018 Reference: Freund et al. Reference: Freund et al.
Date: January 16th, 2020 Reference: Troponin Testing and Coronary Syndrome in Geriatric Patients With Nonspecific Complaints: Are We Overtesting? Andrew Huang: Andy is […] The post SGEM#280: This Old Heart of Mine and Troponin Testing first appeared on The Skeptics Guide to Emergency Medicine. Reference: Wang et al.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. In fact, Kosuge et al. Stein et al. This is a paper worth reading : Marchik et al. What do you think?
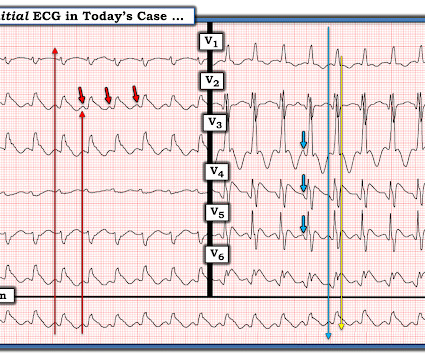
1] But there are multiple other abnormalities that make this ECG diagnostic of Occlusion MI, localized likely to the right coronary artery: 1. Systematic review and meta-analysis of diagnostic test accuracy of ST-segment elevation for acute coronary occlusion. Nikus et al. Kontos et al. Kontos et al. Bischof et al.
The latest is Langlois-Carbonneau et al. But like many similar studies, the study was small (one year at one centre with no indication of the incidence of acute coronary occlusion), and it used as the gold standard the final cardiologist interpretation of the ECG - not the patient outcome! But according to Langlois-Carbonneau et al.,
Date: May 24th, 2022 Reference: Broder et al. Guidelines for Reasonable and Appropriate Care in the EmergencyDepartment (GRACE) 2: Low-Risk, Recurrent Abdominal Pain in the EmergencyDepartment. Date: May 24th, 2022 Reference: Broder et al. Reference: Broder et al.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergencydepartment with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. Amsterdam et al. Alencar et al. Lupu et al. But does this matter? Circulation 2014 2.
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] It’s judicious, then, to arrange for coronary angiogram. link] [1] Mirand, D.
Additional architectural changes include systolic anterior motion of the mitral valve, endothelial dysfunction at the level of the coronary arterial bed, and ventricular diastolic dysfunction. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. It is spread to V2 and V3. References Naidu, S.
It has been said that it can take 17 years for 14% of research to reach the patients’ bedside ( Morris et al 2011 ). Talk I: Knowledge Translation in the Digital Age The first talk was on knowledge translation (KT) in the digital age. A number of examples of the KT problem were provided.
emergencydepartments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. References Tsao CW, et al. Benjamin EJ, et al. Kimblad H, et al. Adult cardiac arrest in the emergencydepartment – A Swedish cohort study. Sakai T, et al. Kudenchuk PJ, et al.
[display_podcast] Date: March 6th, 2018 Reference: Zahed et al. Guest Skeptic: Dr. Justin Morgenstern is an emergency physician and the Director of Simulation Education at Markham Stouffville Hospital in Ontario. display_podcast] Date: March 6th, 2018 Reference: Zahed et al. Reference: Zahed et al. AEM March 2018.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). link] [1] Zachary et al. Utility of the history and physical examination in the detection of Acute Coronary Syndromes in emergencydepartment patients. 2] Costanzo, L. Physiology. 3] Parham, W.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" Chris Mondie of the Newark Beth Israel Emergency Medicine Residency sent case 1 below of a 100% LM occlusion. Widimsky P et al.
If you were working in a busy emergencydepartment, would you like to be interrupted to interpret these ECGs or can these patients safely wait to be seen because of the normal computer interpretation? Emergent cardiac outcomes in patients with normal electrocardiograms in the emergencydepartment. Am J Emerg Med.
Below is the version standardized by PM Cardio app Meyers interpretation: Findings are specific for posterior (and also likely inferior) wall transmural acute infarction, most likely due to acute coronary occlusion (OMI). Most OMI have a peak Troponin T over 1000 ng/L [reference: Baro R et al. Clinical Cardiology 2019.
Autopsy shows coronary atherosclerosis and marked cardiomegaly with a thickened left ventricular wall. References : System-Level Process Change Improves Communication and Follow-Up for EmergencyDepartment Patients With Incidental Radiology Findings. Baccei SJ et al. Tyler W et al. Volume 80, no.
Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy.
It is commonly used in EmergencyDepartments, especially in febrile and possibly infectious patients. Schillinger M, Domanovits H, Bayegan K, Hölzenbein T, Grabenw ö ger M, Thoenissen J, et al. Posted by: Lakshay Chanana ST4 Trainee Royal Infirmary of Edinburgh Department of Emergency Medicine Edinburgh Scotland @EMDidactic
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
Upon arrival at the receiving emergencydepartment, however, she precipitously degenerated into VF and could not be resuscitated. In most cases, rather, the culprit is gross ischemia due to myocardial infarction, cardiomyopathy, or advanced coronary artery disease. Unfortunately, a post-conversion 12 Lead was not acquired.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergencydepartment with 2 days of heavy substernal chest pain and nausea. Serial ECGs enhance the diagnosis of acute coronary syndrome. Bigger et al. Annals of Emergency Medicine , 31 (1), 3–11.
Background and Context Contrast-enhanced computed tomography (CECT) is of paramount importance in the emergencydepartment (ED) due to its indispensable role in facilitating precise diagnostic outcomes. 16 In a study conducted by Millet et al. link] Bellolio MF, Heien HC, Sangaralingham LR, et al. West J Emerg Med.
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergencydepartment at around 3 AM complaining of chest pain onset around 9 PM the evening prior. Guagliumi, G., Iwaoka, R.
2, 3 Biliary POCUS can help decrease patient length of stay in the EmergencyDepartment. Video 3: Coronary approach to the gallbladder POCUS Findings Sonographically, the gallbladder is situated in the right upper quadrant as an elongated pear-shaped organ on the inferior surface of the liver. Acad Emerg Med. Ultrasound.
AslangerE A 65-year-old gentleman presented to the emergencydepartment after experiencing two recent ICD shocks in the preceding hours. A recent angiogram report indicated a totally occluded left anterior descending artery (LAD) and right coronary artery (RCA), with 30-40% narrowings in the left circumflex artery (LCx).
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergencydepartment with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. Akkerhuis KM, et al. Gottlieb SO, et al. Jernberg T, et al.
Many conditions outside of acute coronary syndrome (ACS) mimic ST-elevation myocardial infarction (STEMI), but only a handful of cases have reported ST-elevations (STE) in the setting of pancreatic inflammation where underlying ACS was excluded. 2 Proposed hypothesis as described by Hsu et al., Click to enlarge.)
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. References Hansen MS, et al. Rogers AM, et al. Cecconi M, et al. Circulation.
Am J Emerg Med. I have here 38 cases of "Computer Normal" ECGs which were critically abnormal and the vast majority are missed acute coronary occlusions (Missed Acute OMI) and most were recognized by the physician. Of the Non-STEMI in our cohort, about 25% will actually have acute coronary occlusion. 2022 Jan;51:384-387.
A 68-year-old male with a past medical history of hypertension, diabetes mellitus, and coronary artery disease with a drug eluting stent placed 2 months ago presents with dizziness and vomiting that began 3 hours ago. References: Gaillard F, Glick Y, Tatco V, et al. 61.4.496 Navi BB, Kamel H, Shah MP, et al. Arch Neurol.
Hgb 11g/dL (110g/L) and leukocytosis, and a mildly elevated troponin (36 ng/L, with normal 1mm STE in aVR due to ACS will require coronary artery bypass surgery for revascularization, the infarct artery is often not the LM, but rather the LAD or severe 3-vessel disease. Harhash AA, Huang JJ, Reddy S, et al. Knotts et al.
I want all to know that, with the right mind preparation, and the use of the early repol/LAD occlusion formula, extremely subtle coronary occlusion can be detected prospectively, with no other information than the ECG. It is not a missed STEMI, but it is a missed coronary occlusion. Fesmire et al. Ann Emerg Med 1998;31(1):3-11.
A 35-year-old male presented to the emergencydepartment complaining of chest pain that started 1.5 5 Studies looking at this phenomenon in the emergencydepartment setting for patients presenting with chest pain are lacking. Dr. Young is an emergency physician at Saint Francis Hospital and Medical Center, Hartford, Conn.
Objective: Based on current evidence, this review article aims to guide the EmergencyDepartment (ED) in providing care for patients with blast injuries. Cardiovascular: Injury: cardiac contusion, wall rupture, tamponade, papillary muscle rupture, valve injury, aortic arch injury, and coronary artery dissection. Nowadly C.D.,
Rather it is due to coronary insufficiency due to a tight left main or 3-vessel disease with inadequate coronary flow. Kurkciyan et al. Data collected included demographics, initial rhythm, EKG, emergencydepartment (ED) CT and outcomes. Kurkciyan et al., In 25 (93%), the initial rhythm was asystole or PEA.
References: Canto JG, Shlipak MG, Rogers WJ, et al. Dorsch MF, Lawrence RA, Sapsford RJ, et al. Presenting complaint among patients with myocardial infarction who present to an urban, public hospital emergencydepartment. Ann Emerg Med 2002; 40:180–6. Uretsky BF, Farquahr DS, Berezin AF, et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















































Let's personalize your content