This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Date: November 22, 2023 Reference: Stopyra et al. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Date: November 22, 2023 Reference: Stopyra et al. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI.
Bogossian et al. (1) Bogossian H, Frommeyer G, Ninios I, Hasan F, Nguyen QS, Karosiene Z, Mijic D, Kloppe A, Suleiman H, Bandorski D, et al. Dodd KW, Elm KD, Dodd EM, Smith SW. Among patients with left bundle branch block, T-wave peak to T-wave end time is prolonged in the presence of acute coronary occlusion.
Date: September 8th, 2021 Reference: Desch et al. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. Date: September 8th, 2021 Reference: Desch et al. The TOMAHAWK Investigators. The TOMAHAWK Investigators.
We’ll keep it short, while you keep that EM brain sharp. Upon further research in the 1970’s, retrospective data from autopsies of those patients showed coronary aneurysms 5 Pathophysiology: Kawasaki Disease is a vasculitis of medium sized arteries.
We’ll keep it short, while you keep that EM brain sharp. A 68-year-old male with a past medical history of hypertension, diabetes mellitus, and coronary artery disease with a drug eluting stent placed 2 months ago presents with dizziness and vomiting that began 3 hours ago. References: Gaillard F, Glick Y, Tatco V, et al.
Here is the case: Report from EMS was witnessed syncope, his son did CPR, but the patient had pulses when EMS arrived. When the patient arrived in the ED, he was still hypotensive in 70s, slowly improving with EMS fluids. Hope you’re doing well! How excited would you have been about this case?" No Chest Pain, but somnolent.
According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. One cannot rely on this feature as a means of detecting changes – subtle, or dramatic – for volatile occlusive coronary thrombus. Here is the LAD after stent placement.
Fire/EMS personnel find her laying supine on the kitchen floor, awake and verbal, although acutely ill. Additional architectural changes include systolic anterior motion of the mitral valve, endothelial dysfunction at the level of the coronary arterial bed, and ventricular diastolic dysfunction. It is spread to V2 and V3.
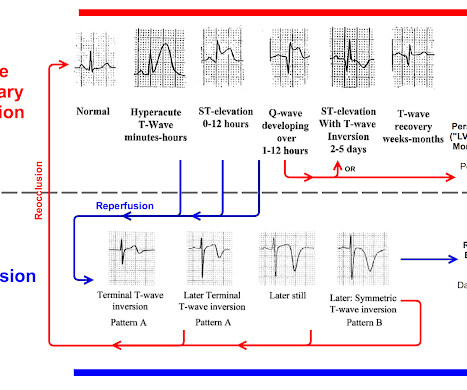
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT. Amsterdam et al. Alencar et al.
EMS was called, and they recorded the following ECG on scene at 13:16: What do you think? Below is the version standardized by PM Cardio app Meyers interpretation: Findings are specific for posterior (and also likely inferior) wall transmural acute infarction, most likely due to acute coronary occlusion (OMI). Clinical Cardiology 2019.
He presented to EMS with extreme pallor, Levine sign, diaphoresis, bilateral arm pain, and an apprehensive sense of doom. It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). link] [1] Zachary et al. Past medical history included HTN, HLD, and MI 10 years prior.
When EMS found her, she was dyspneic and diaphoretic. Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ).
EMS obtained the following vital signs: pulse 50, respiratory rate 16, blood pressure 96/49. It appears EMS obtained two EKGs, but unfortunately these were not saved in the medical record. The EMS crew was only BLS certified, so EKG interpretation is not within their scope of practice. This is not the case.
The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Takotsubo should be a diagnosis of exclusion after angiography reveals no obstructive coronary disease, and repeat Echo displays left ventricular recovery. Furthermore, pertinent electrolyte values (e.g. potassium) were within normal parameter.
Extracorporeal membrane oxygenation Of patients with out-of-hospital cardiac arrest presenting to the ED in refractory VF, a majority have significant coronary artery disease, much of which is amenable to percutaneous coronary intervention. References Tsao CW, et al. Benjamin EJ, et al. Kimblad H, et al.
Date: May 24th, 2022 Reference: Broder et al. Date: May 24th, 2022 Reference: Broder et al. Reference: Broder et al. Guidelines for Reasonable and Appropriate Care in the Emergency Department (GRACE) 2: Low-Risk, Recurrent Abdominal Pain in the Emergency Department. There can be many presentations for low-risk abdominal pain.
Written by Jesse McLaren A previously healthy 60 year old developed exertional chest pain with diaphoresis, and called EMS. Here’s the EMS ECG, digitized with PM cardio. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion. Take home 1.
Pillai, MBBS (@sspillai01, EM Resident Physician, University of Kentucky) and Christopher N. 2 In response to the constrained availability of contrast media, emergency medicine (EM) and radiology departments were compelled to enact modifications in their imaging techniques. 16 In a study conducted by Millet et al. 11 Table 1.
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. 4] Baranchuk, A, et al. BP 110/67 HR 68 RR 14 (non-labored) SpO2 95 RA Physical exam revealed slight pallor and diaphoresis. Attached is the first ECG. 2] Surawicz, B.
It shows that on a 7 day angiogram, only 58% of re-occlusions were symptomatic: Ohman EM, Califf RM, Topol EJ et al. It is important to recognize that coronary thrombosis is dynamic , with spontaneous opening and lysing of the thrombus in the infarct-related artery (we all have endogenous tPA and plasmin to lyse thrombi).
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chest pain. Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. Smith adds to our knowledge of this syndrome.
He awoke from sleep with crushing central chest pain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. Angiographic and clinical characteristics of patients with unstable angina showing an ECG pattern indicating critical narrowing of the proximal LAD coronary artery. de Zwaan C.,
EMS arrived and recorded this ECG: What do you think? I have here 38 cases of "Computer Normal" ECGs which were critically abnormal and the vast majority are missed acute coronary occlusions (Missed Acute OMI) and most were recognized by the physician. So this study is worthless and must be ignored. Litell JM, Meyers HP, Smith SW.
Queen of Hearts now thinks that this one looks like posterior OMI, since the STD does appear worst in V3-4: None of this seems to have been understood by the EM doctor or the cardiologist who was consulted. The De Winter ECG pattern: morphology and accuracy for diagnosing acute coronary occlusion: systematic review. 2009;95:1701–1706.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al.
The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. With both EMS and ED computer interpretations reading ‘STEMI’, the emergency physician activated the cath lab. With both EMS and ED computer interpretations reading ‘STEMI’, the emergency physician activated the cath lab.
Learn about the Smith-Modified Sgarbossa Criteria for Diagnosis of OMI Paced Rhythm: Dodd, Meyers, Smith, et al. Electrocardiographic diagnosis of acute coronary Occlusion Myocardial Infarction in ventricular paced rhythm using the modified Sgarbossa criteria. Annals of Emergency Medicine 2021. Great job!!
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. En route, EMS administered aspirin 325mg by mouth, but withheld nitroglycerin due to initial hypotension. Answer below in the still shot.
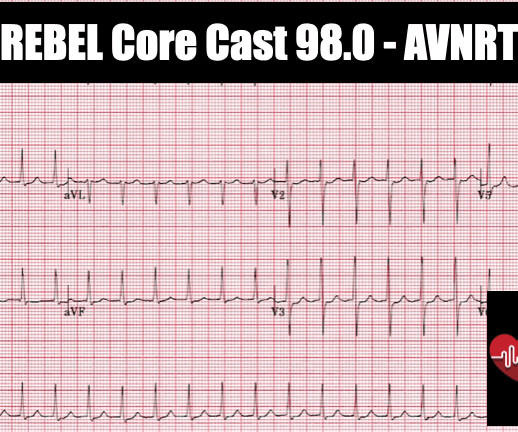
Amal Mattu’s ECG Blog has an excellent review of AVNRT vs. VT and REBEL EM reviews the sensitivity and specificity of various algorithms. PMID: 2022022 Appleboam A et al. PMID: 1595533 Ben Yedder N et al. PMID: 21329868 Carlberg DJ et al. A new approach to the diagnosis of regular wide complex tachycardia. Lancet 2015.
The case below was contributed by Pendell Meyers, an EM G1 at Mt. Here is a link to the case report: Dynamic T-wave inversions in the setting of left bundle branch block Though Wellens' syndrome was described in the LAD territory, I have shown cases demonstrating that it occurs in any coronary distribution. Meyers HP et al.
It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chest pain. This is step 4 : relying on the first troponin level to rule out acute coronary occlusion. 4] CT revealed no dissection but extensive coronary atherosclerosis. J of Emerg Med 2021.
Meyers et al. Accuracy of OMI findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardial infarction. Aslanger et al. DIagnostic accuracy oF electrocardiogram for acute coronary OCClusion resulTing in myocardial infarction (DIFOCCULT study). Lemkes et al. Bergmark et al.
et al, Emergency Medicine Clinical Essentials ed 2. Eye Emergencies, in Tintinalli J et al (eds): Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, Seventh Edition New York City: McGraw-Hill 2016 (Ch) 241 Guluma K, Lee JE. Ophthalmology, in Marx J et al (eds): Rosens Emergency Medicine: Concepts and Practice, ed 9.
This post was written by Tarissa Lai, one of our outstanding EM residents at Hennepin County Medical Center, with comments by Steve Smith and Dan Lee. female with HTN, HLD, diabetes, ESRD on dialysis is brought in by EMS with sudden onset, left -sided chest pain for the past four hours. Case A 30 something y.o.
This " imbalance of precordial T waves" is not seen very often — and in the “right” clinical setting, has been associated with recent OMI from a LCx culprit artery ( See Manno et al: JACC 1:1213, 1983 — and the July 17, 2013 post by Salim Rezaie in ALiEM ).
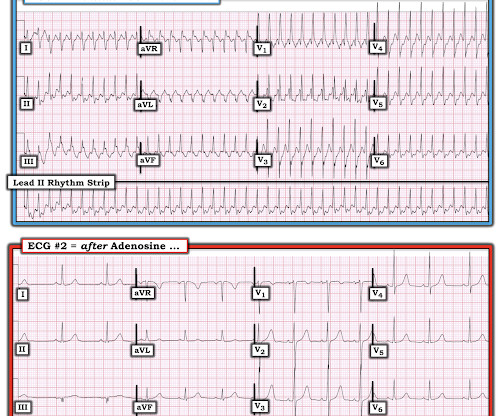
Read about Fascicular VT here: Idiopathic Ventricular Tachycardias for the EM Physician Case Continued He was completely stable, so adenosine was administered. SVT misdiagnosed as panic disorder Lessmeier TJ, Gamperling D, Johnson-Liddon V, et al. Lessmeier et al. Admission and referral to electrophysiology is always indicated.
The patient had this ECG recorded at 7 minutes after registration at triage as a walk-in (not by EMS): What do you think? Reference: • Writing Committee, Kontos MC, de Lemos JA, et al. Here is the case in total. 62 yo with severe (10/10) CP of 3.5 hours duration. BP is 186/106. This is diagnostic of posterolateral OMI.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Essentially, we are using the troponin assay to find patients with ACO who may be benefited by coronary interventions or risk factor modification. Cardiol Rev.
He reported to EMS a medical history of GERD only. V2 – in the final EMS ECG the ST segment was baseline. V3 – in the final EMS ECG the ST segment was still slightly depressed. Cardiology admitted him for observation with plans for next-day coronary angiogram. However, in this context (i.e. 1] Driver, B. 1] Driver, B.
EMS finds him supine, alert and oriented, and without any gross distress. Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. Crew members note residual pallor and clammy skin. 3] Meyers, H.
David Didlake, NRP, APRN, ACNP-BC @DidlakeDW Expert analysis provided by Dr. Ken Grauer [link] @ekgpress EMS is called to the main reception area of a retirement center where an elderly female is found down, unconscious and unresponsive. She has a palpable pulse at the radial arteries, bilaterally, with shallow respirations.
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] It’s judicious, then, to arrange for coronary angiogram. link] [1] Mirand, D.
Article: Branch KHR et al. Indication for emergency invasive coronary angiography or had coronary angiography within 1 hour of arrival. Known obstructive coronary artery disease or known coronary stent. References: Branch KHR et al. appeared first on REBEL EM - Emergency Medicine Blog. Resus 2023.
About 2 hours later the patient arrived at a PCI-capable center and repeat ECG was obtained: The transferring EMS crew noted “runs of VT” during transport. Serial ECGs enhance the diagnosis of acute coronary syndrome. Bigger et al. Sadowski ZP, Alexander JH, Skrabucha B, et al. In fact, use of antidyrhythimcs (e.g.,
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content