This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. Furthermore, if this occurs at all, it is a rare event. years, with the interval as long as 12 or 18 years in some studies.
Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? AEM June 2022.
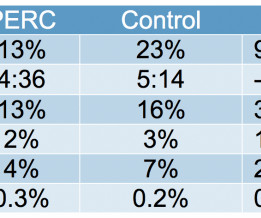
[display_podcast] Date: May 16, 2018 Reference: Freund et al. Effect of the Pulmonary Embolism Rule-Out Criteria on Subsequent Thromboembolic Events Among Low-Risk Emergency Department Patients: The PROPER Randomized Clinical Trial. display_podcast] Date: May 16, 2018 Reference: Freund et al. Reference: Freund et al.
Thank you to Dr. Manrique Umana for inviting me and the conference organizers for putting on such an amazing and educational event. Thank you to Dr. Manrique Umana for inviting me and the conference organizers for putting on such an amazing and educational event. A number of examples of the KT problem were provided.
Does that normal troponin and ECG obviate the need for cardiology consultation for my patient with a concerning story for acute coronary syndrome? Knack SKS, Scott N, Driver BE, Pet al. Thiruganasambandamoorthy V, Kwong K, Wells GA, et al. Freund Y, Cachanado M, Aubry A, et al. Penaloza A, Verschuren F, Meyer G, et al.
Beats 9-12 : Continuation of the previously described events, all inducible by the pause (and thus, prolongation of refractoriness) created by the PVC of Beat 8. The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Beat 4 abruptly halts this repetitious cycle via Peel Back. References Chiale, P. Saini, A.,
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
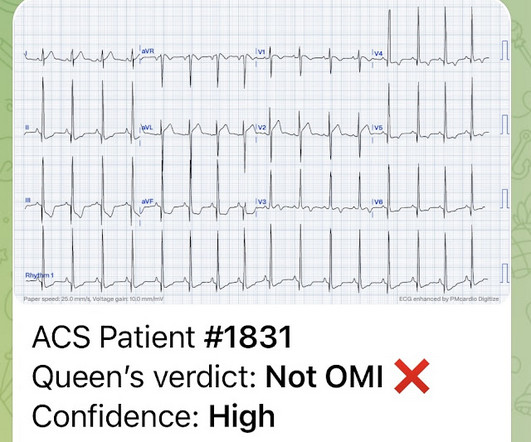
Coronaries were clean. Not OMI with High Confidence Click here to sign up for Queen of Hearts Access We showed that the Queen of Hearts decreases false positive cath lab activations: 1) Published recently in Prehospital Emergency Care Baker PO et al. 2) To be presented at AHA conference in Chicago in 2 weeks: Sharkey SW et al.
A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. Lemkes JS, et al. Total coronary occlusion, if very brief, may have minimal infarction and yet be very dangerous. Am Heart J. 2000;139:430–436. Eur Heart J [Internet].
GLP-1 agonists are also associated with improved ejection fraction, coronary blood flow, and cardiac output while reducing the risk of cardiovascular events, infarction size, and all-cause mortality. Adverse events are common in those using GLP-1 agonists, but the vast majority of these are minor. What are the complications?
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So the patient had a transient acute coronary occlusion that spontaneously reperfused but is at risk for reocclusion. Deutch et al.
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. Whether this represents a potential acute cardiac event would depend on the history, comparison with prior tracings and serial tracings. 4] Baranchuk, A, et al.
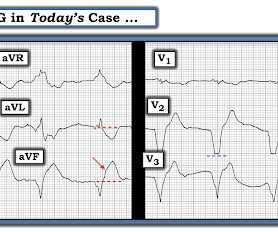
Acute MI per se usually does not depress cardiac function and blood pressure enough to cause syncope ( Mostafa et al — J Com Hosp Intern Med Perspect 13(4):9-12, 2023 - ). The initial ECG in today's case was recognized as definitely abnormal — but the question arose as to whether this ECG indicated old infarction vs a new acute event.
The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA.
Heitner et al. We know that even high-sensitivity troponin may not exceed the "normal" range for a period of hours in certain patients with acute coronary occlusion. The PDA plaque was also bulky, but was not described as inflamed or ulcerated. DOI:10.1161/CIRCINTERVENTIONS.118.007305), DOI:10.1161/CIRCINTERVENTIONS.118.007305),
Takotsubo is a sudden event, not one with crescendo angina. Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!!
It shows that on a 7 day angiogram, only 58% of re-occlusions were symptomatic: Ohman EM, Califf RM, Topol EJ et al. It is important to recognize that coronary thrombosis is dynamic , with spontaneous opening and lysing of the thrombus in the infarct-related artery (we all have endogenous tPA and plasmin to lyse thrombi).
A Short Comment on PIRP and T Waves: Oliva et al found a strong association of myocardial rupture with postinfarction regional pericarditis. Another possible cause of pseudonormalization of T waves mentioned many times on this blog is the pseudonormalization caused by re-occlusion of an infarct related reperfused coronary artery.
16 In a study conducted by Millet et al. A retrospective study done in May 2023, by Shaish et al 24 showed a 30 % reduction in accuracy of NCCT compared to CECT in a study done among 201 adult ED patients with abdominal pain. link] Bellolio MF, Heien HC, Sangaralingham LR, et al. References Abelson R. The New York Times.
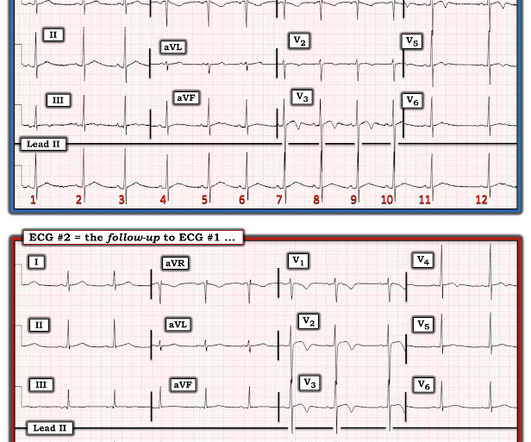
Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.) have perfect coronary flow by the time of angiogram. The fatter-than-it-should-be T wave in lead aVL is the mirror image opposite picture of the ST-T wave in lead III ==> reciprocal change that strongly suggests a recent ( if not still ongoing acute ) event.
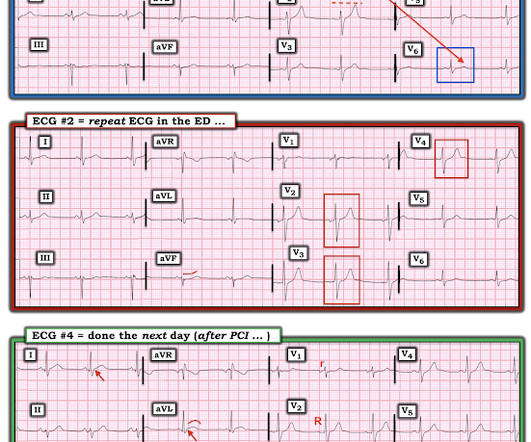
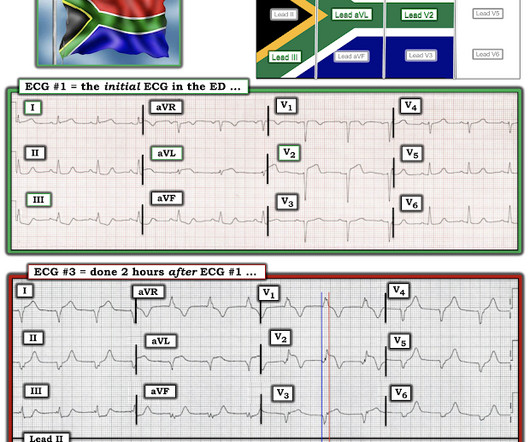
Lemkes et al. A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. And dynamic ST-T wave changes between ECG #1 and ECG #2 confirm an acute event in progress. Eur Heart J 2018. Full text link. Am Heart J.
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published. ST depression that is maximal in leads V2-to-V4.
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronary artery disease and myocardial infarctions. PLUS — Today's patient is an older woman with known severe coronary disease who presented with new chest pain. She's had multiple PCI procedures.
The De Winter ECG pattern: morphology and accuracy for diagnosing acute coronary occlusion: systematic review. Hayakawa A, Tsukahara K, Miyagawa S, et al. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardial infarction patients. 2009;95:1701–1706. As per Drs.
I was not worried for a coronary etiology. Under most circumstances — this combination of ECG findings would point to an acute event. PEARL #3: The pathophysiologic mechanism for producing amphetamine-induced acute MI is unclear ( Bazmi et al — SQUMJ 17(10); e31-37, 2017 — and — Sinha et al — Case Rep Cardiol, 2016 ).
Backus BE, Six AJ, Kelder JC, et al. Moumneh T, Sun BC, Baecker A, et al. Identifying patients with low risk for acute coronary syndrome without troponin testing: validation of the HEAR score. Shah ASV, Anand A, Sandoval Y, et al. Patel J, Alattar F, Koneru J, et al. Gulati M, Levy P, Mukherjee D, et al.
STEMI criteria is bad at differentiating between normal variant and acute coronary occlusion or reperfusion, and initial troponin levels don't differentiate between occlusive and non-occlusive MI 3. the presence of J waves from early repolarization doesn’t rule out an acute coronary occlusion 4. McLaren et al, including Meyers/Smith.
Learn about the Smith-Modified Sgarbossa Criteria for Diagnosis of OMI Paced Rhythm: Dodd, Meyers, Smith, et al. Electrocardiographic diagnosis of acute coronary Occlusion Myocardial Infarction in ventricular paced rhythm using the modified Sgarbossa criteria. Annals of Emergency Medicine 2021. Figure-1: The 2nd ECG in today's case. (
The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
Meyers et al. Accuracy of OMI findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardial infarction. Aslanger et al. DIagnostic accuracy oF electrocardiogram for acute coronary OCClusion resulTing in myocardial infarction (DIFOCCULT study). Lemkes et al. Bergmark et al.
Herzog et al. Khan et al. We need to remember that not all patients with acute ( or recent ) MI have chest pain with their event. ECG interpretation needs to be done in isolation and then applied to the patient, and this way AI can help identify patients at risk of missed occlusions References 1. Circulation 2007 2.
Moreover, the research which appears to confirm this idea was indeed in relation to the circumflex, but they did not study Occlusion ; rather, they studied asymptomatic coronary disease. I showed conclusively that this is a common finding in normal ECGs, though it is more common in LAD Occlusion than in norml variant STE.
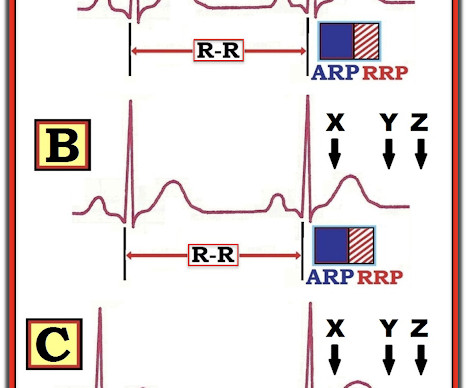
A coronary angiogram was done that did not show significant coronary artery disease. Events in Panel B — suggest a different clinical situation. Most Torsades is the result of a pause-dependent effect that predisposes to development of the malignant arrhythmia ( Dohadwala et al — Heart Rhythm Case Rep 3(2):115-119, 2017 ).
Wellens pattern is a term which refers to coronary reperfusion morphology in the anterior leads) The best answer is because the entire gestalt of the ECG shows acute right heart strain instead, and just does not look like Wellens after you've seen Wellens hundreds of times. Stein et al. This is a paper worth reading : Marchik et al.
Sequence of events in angina at rest: Primary reduction in coronary flow. Normalization of abnormal T waves in ischemia. Arch Intern Med. 1976 Apr;136(4):391-5. Chierchia S, Brunelli C, Simonetti I, Lazzari M, Maseri A. Circulation. 1980 Apr;61(4):759-68. Simons A, Robins LJ, Hooghoudt TE, Meursing BT, Oude Ophuis AJ.
Karwowski et al showed that only 64% of 4581 STEMIs had TIMI 0 flow on angiogram. [25] 25] Stone et al found that 72% have TIMI 0 or 1 flow. [26] 26] Finally, Cox et al found that 80% had TIMI 0, 1, or 2.27 Karwowski et al showed that only 64% of 4581 STEMIs had TIMI 0 flow on angiogram. [25] Pol Arch Intern Med.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion). Aspirin 81 mg daily.
The criteria of Armstrong et al. LVH can mimic an acute anterior coronary occlusion (ACO) on the ECG. One retrospective analysis by Armstrong et al. Electrocardiographic left ventricular hypertrophy in chest pain patients: Differentiation from acute coronary ischemic events. AT, Jaffa EJ, et al. J Emerg Med.
Ct coronary angiogram showed normal coronary arteries. Smith note: I think CT coronary angiogram is reasonable with the elevated troponins and symptoms. The Cardiorespiratory Implications of Ultra-marathon Bjørkavoll‐Bergseth et al. Paana et al. He was diagnosed with mild AKI which resolved. ng/L; 3 hours, 38.3
CASE #2: I am more disturbed by learning of the events associated with the ECG in Case #2. NOTE: For illustrative purposes — I’ve adapted Figure-1 from the original manuscript by deWinter et al, published in this 2008 NEJM citation. de Winter et al in N Engl J Med 359:2071-2073, 2008. See text ).
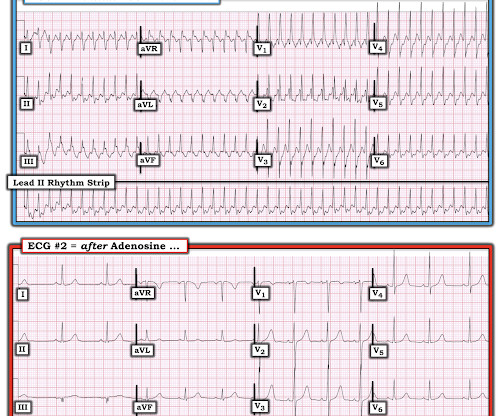
mg/kg IV is administered if no response is seen and no significant drug-induced adverse event occurs. SVT misdiagnosed as panic disorder Lessmeier TJ, Gamperling D, Johnson-Liddon V, et al. Lessmeier et al. I’ll add here 2 more reference links on the subject — by Brugada; Diez — and — by Tondo et al. mg/kg IV over 2 min.
Acute 100% coronary occlusion can be VERY subtle on the ECG. Hillinger et al. IF ever in doubt about whether an acute event may be ongoing — Repeat the ECG within 10-to-15 minutes ( since dynamic ST-T wave changes during an actively evolving event may occur with surprising rapidity ). Learning Points: 1.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content