This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
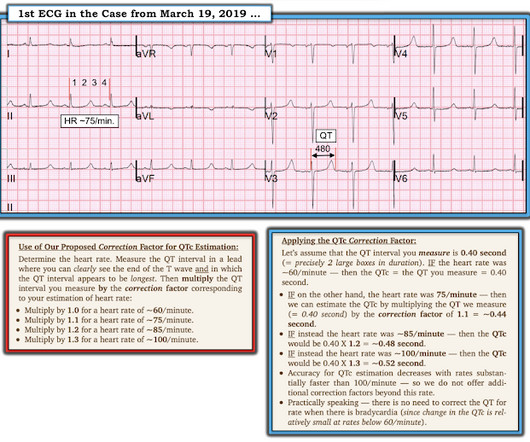
Date: November 22, 2023 Reference: Stopyra et al. Date: November 22, 2023 Reference: Stopyra et al. A 12-lead electrocardiogram (ECG) demonstrates ST elevations in leads II, III, and aVF with ST depressions in leads I and aVL and the team begins transport to the nearest percutaneous coronary intervention (PCI) capable hospital.
Intermediate-risk patients may be further stratified based on recent stress testing or coronary angiogram findings plus a modified HEART or Emergency Department Assessment of Chest Pain (EDACS) score. Encourage your ED to set up an algorithm that you can follow based on your laboratory’s assay. She does not smoke.
Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. Thus, the lumen observed may actually still be the same size as the original, normal lumen.
A 45-year-old male with a history of chronic obstructive pulmonary disease (COPD), asthma, amphetamine and tetrahydrocannabinol (THC) use, and coronary vasospasm presented to triage with chest pain. During assessment, the patient reported that a left heart catheterization six months prior indicated spasms but no coronary artery disease.
Bogossian et al. (1) Bogossian H, Frommeyer G, Ninios I, Hasan F, Nguyen QS, Karosiene Z, Mijic D, Kloppe A, Suleiman H, Bandorski D, et al. Among patients with left bundle branch block, T-wave peak to T-wave end time is prolonged in the presence of acute coronary occlusion. T-waves are quite tall and possibly peaked (HyperK?),
Date: September 23, 2024 Reference: Essat et al. The patient has no specific risk factors for acute coronary syndrome (ACS) or dissection. Reference: Essat et al. Diagnostic Accuracy of D-Dimer for Acute Aortic Syndromes: Systematic Review and Meta-Analysis. There are no abnormalities in the blood work, ECG, or chest x-ray.
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. The original term " benign early repolarization" has fallen out of favor since the seminal paper by Haïssaguerre et al.
Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Reference: McGinnis et al.
Why Was Cardiac Cath Negative for Coronary Disease? As noted by Dr. Nossen — this patient qualified as MINOCA ( M yocardial I nfarction with N on- O bstructive C oronary A rteries ) — since troponin was positive on his 2nd admission, yet there was no evidence of obstructive coronary disease on cath.
Extracorporeal membrane oxygenation Of patients with out-of-hospital cardiac arrest presenting to the ED in refractory VF, a majority have significant coronary artery disease, much of which is amenable to percutaneous coronary intervention. Out-of-hospital cardiac arrest is a commonly encountered entity in U.S.
The latest is Langlois-Carbonneau et al. But like many similar studies, the study was small (one year at one centre with no indication of the incidence of acute coronary occlusion), and it used as the gold standard the final cardiologist interpretation of the ECG - not the patient outcome! But according to Langlois-Carbonneau et al.,
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients.
[display_podcast] Date: October 19th, 2017 Reference: Hofmann et al. display_podcast] Date: October 19th, 2017 Reference: Hofmann et al. Studies have shown that oxygen can cause vasoconstriction, increase blood pressure and decrease coronary artery blood flow ( Kones et al AM J Med 2011). NEJM Sept 2017. NEJM Sept 2017.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Essentially, we are using the troponin assay to find patients with ACO who may be benefited by coronary interventions or risk factor modification.
Author: Brit Long, MD (@long_brit) // Reviewed by Alex Koyfman, MD (@EMHighAK) The American Heart Association 2023 Guideline for managing cardiac arrest or life-threatening toxicity due to poisoning was recently released. This post will focus on the key parts of the guideline that affect ED evaluation and management. Top 10 Take Home Pearls 1.
Article: Branch KHR et al. Indication for emergency invasive coronary angiography or had coronary angiography within 1 hour of arrival. Known obstructive coronary artery disease or known coronary stent. References: Branch KHR et al. Advanced imaging post-arrest is a possible modality to achieve this end.
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] It’s judicious, then, to arrange for coronary angiogram. Does the ECG normalize?
Date: January 16th, 2020 Reference: Troponin Testing and Coronary Syndrome in Geriatric Patients With Nonspecific Complaints: Are We Overtesting? Date: January 16th, 2020 Reference: Troponin Testing and Coronary Syndrome in Geriatric Patients With Nonspecific Complaints: Are We Overtesting? Reference: Wang et al.
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT. But does this matter?
1] But there are multiple other abnormalities that make this ECG diagnostic of Occlusion MI, localized likely to the right coronary artery: 1. Systematic review and meta-analysis of diagnostic test accuracy of ST-segment elevation for acute coronary occlusion. Nikus et al. Kontos et al. Kontos et al. Bischof et al.
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. Steve Smith [link] @SmithECGblog A 72 y/o Male experiences a syncopal episode while seated. Crew members note residual pallor and clammy skin.
Zeymer HT et al. The benefits of this strategy may be outweighed by the risk of the device-related complications (i.e. bleeding, stroke, limb ischemia, and hemolysis). The evidence for this practice has been sparse until now. Extracorporeal Life Support in Infarct-Related Cardiogenic Shock. Control: 53.4% D ECLS: 18.2% Control 8.7%
Does that normal troponin and ECG obviate the need for cardiology consultation for my patient with a concerning story for acute coronary syndrome? Coming into triage, I see a young man—Georgian-speaking—bracing himself with a hand against the wall and holding his lower abdomen.
Additional architectural changes include systolic anterior motion of the mitral valve, endothelial dysfunction at the level of the coronary arterial bed, and ventricular diastolic dysfunction. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. It is spread to V2 and V3.
Paper: Van de Werf, F et al. STREAM-2: Half-Dose Tenecteplase or Primary Percutaneous Coronary Intervention in Older Patients With ST-Segment-Elevation Myocardial Infarction: A Randomized, Open-Label Trial. neoplasm, aneurysm, intracranial or spinal surgery) or recent trauma to head or cranium (i.e.
One cannot rely on this feature as a means of detecting changes – subtle, or dramatic – for volatile occlusive coronary thrombus. Discussion When the QRS is normal, is the encountered ST/T changes that beget suspicion for LAD ACS (as in both of these cases) the result of occlusive coronary thrombus, or simply a normal variant?
The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Takotsubo should be a diagnosis of exclusion after angiography reveals no obstructive coronary disease, and repeat Echo displays left ventricular recovery. A 12 Lead ECG was recorded secondary to bizarre telemetry findings at bedside.
In fact, Kosuge et al. showed that among patients with either acute coronary syndrome or acute pulmonary embolism and negative T waves in the precordial leads (V1-V4), that inverted T waves in leads III and V1 were present in only 1% of patients with acute coronary syndrome and 88% of patients with pulmonary embolism. “The
[display_podcast] Date: May 16, 2018 Reference: Freund et al. display_podcast] Date: May 16, 2018 Reference: Freund et al. Reference: Freund et al. Effect of the Pulmonary Embolism Rule-Out Criteria on Subsequent Thromboembolic Events Among Low-Risk Emergency Department Patients: The PROPER Randomized Clinical Trial.
Cardiology admitted him for observation with plans for next-day coronary angiogram. A 56 y/o Male called 911 from his hotel room in the early morning hours after abruptly awakening from sleep with crushing chest discomfort and difficulty breathing. He reported to EMS a medical history of GERD only. He left AMA and is lost to follow-up.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" She had a proven 100% Left Main occlusion No ST shift in aVR This pattern of RBBB/LAFB was also the most common pattern in Fiol et al.
Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ). What do you do clinically when the ECG looks like this?
It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). Upon contrast injection of the LMCA, the patient deteriorated, as the LMCA was severely diseased and flow to all coronary arteries ( LAD, LCx and RCA ) was compromised. He was taken immediately to the cath lab.
The proof of this is that only 5% of patients enrolled had acute coronary occlusion. Lemkes JS, Janssens GN, van der Hoeven NW, et al. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. We at Hennepin recently published this study Sharma et al. This study failed to do so. 5% vs. 58%!! 5% vs. 58%!!
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). link] [1] Zachary et al. Utility of the history and physical examination in the detection of Acute Coronary Syndromes in emergency department patients. ECG's are difficult. 2] Costanzo, L. Physiology.
A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. Lemkes JS, et al. Total coronary occlusion, if very brief, may have minimal infarction and yet be very dangerous. Pattern A evolves into Pattern B. Am Heart J.
In most cases, rather, the culprit is gross ischemia due to myocardial infarction, cardiomyopathy, or advanced coronary artery disease. Moreover, front office staff advise that she is a new tenant, and thus have nothing more to offer than a name and assigned apartment number. In general, monomorphic VT has a single, stable QRS morphology.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. Because the lungs receive 100% of cardiac output, it has been hypothesized that a lower dose of thrombolytic therapy may still be effective with a better safety profile [3][4]. REBEL Cast Ep123: Reduced-Dose Systemic Peripheral Alteplase in Massive PE?
Coronaries were clean. Not OMI with High Confidence Click here to sign up for Queen of Hearts Access We showed that the Queen of Hearts decreases false positive cath lab activations: 1) Published recently in Prehospital Emergency Care Baker PO et al. 2) To be presented at AHA conference in Chicago in 2 weeks: Sharkey SW et al.
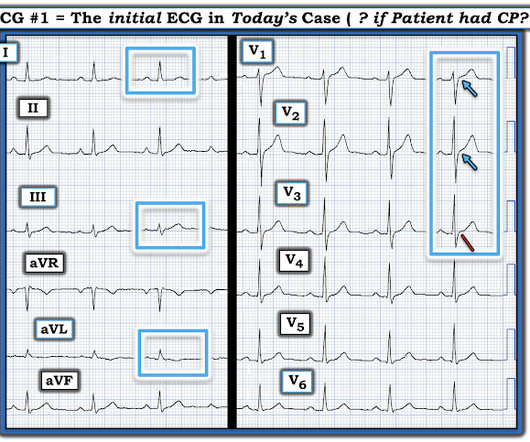
Below is the version standardized by PM Cardio app Meyers interpretation: Findings are specific for posterior (and also likely inferior) wall transmural acute infarction, most likely due to acute coronary occlusion (OMI). Most OMI have a peak Troponin T over 1000 ng/L [reference: Baro R et al.
[display_podcast] Date: March 6th, 2018 Reference: Zahed et al. display_podcast] Date: March 6th, 2018 Reference: Zahed et al. He is the creator of the excellent #FOAMed project called First10EM.com Case: A 77-year-old woman with known coronary artery disease is on clopidogrel and aspirin because of a stent placed four month ago.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content