This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background: Primary PCI is the recommended reperfusion strategy in patients with STEMI and should be initiated within 2 hours after first medical contact. Paper: Van de Werf, F et al. In non-PCI-capable hospitals this goal is not always achievable due to delays in transfer. Primary PCI: 95.7% Primary PCI: 95.7% Primary PCI: 78.4%
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation. The TOMAHAWK Investigators. first appeared on The Skeptics Guide to Emergency Medicine.
Date: February 1, 2023 Reference: Wolfrum et al. Date: February 1, 2023 Reference: Wolfrum et al. The nurses started CPR immediately and place pads before you even arrived. A post-arrest ECG doesn’t show any signs of STEMI. Temperature Control After In-Hospital Cardiac Arrest: A Randomized Clinical Trial. Circulation.
Zeymer HT et al. Did they get bystander CPR? References: Zeymer HT et al. The benefits of this strategy may be outweighed by the risk of the device-related complications (i.e. bleeding, stroke, limb ischemia, and hemolysis). The evidence for this practice has been sparse until now. Control: 53.4% D ECLS: 18.2% Control 8.7%
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiac arrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. Finally, head-up CPR (which was not used here), makes for better resuscitation.
See this paper by Widimsky et al, which shows the high association of RBBB, especially with LAFB, with LAD occlusion. Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiac arrest with unrecognized STEMI, died.
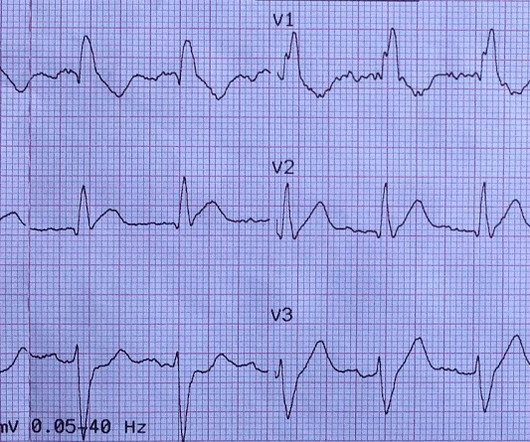
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
Medics found her apneic and pulseless, began CPR, and she was found to be in asystole. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Kurkciyan et al.
This is an extremely important topic especially for EMS systems that are implementing High Performance CPR , because it is very predictable that you are going to see a lot more patients with return of pulses in the field, and if you don’t have a plan, lots of things can go wrong before arriving at the hospital.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
It was witnessed, and CPR was performed by trained individuals. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The following 12-lead ECG was recorded at 11 minutes after ROSC. see below). see below).
Article Summary by Sarah Fabiano, MD, FACEP, FAAEM Lyng JW, Braithwaite S, Abraham H, et al. Air medical transport has been utilized in multiple hospital based programs including trauma, STEMI, and stroke. Cardiac arrest has been proven difficult in flight, but research is still needed with mechanical CPR machines.
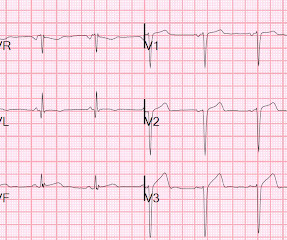
It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. This ECG was recorded prehospital, and the computer read STEMI, so the medics activated the cath lab: What do you think? The ECG is consistent with high lateral STEMI. Called 911.
Raitt MH, et al. cm diameter in the apex The presence of thrombus led the clinicians to state that this was a "late presentation STEMI." It does take some time for thrombus to form, but the EKG and the troponin profile show that this was NOT a late presentation STEMI. Methods: Oliva et al. (94) Methods: Oliva et al.
He underwent CPR, and regained a pulse after epinephrine, with an organized narrow complex rhythm at 140, but still with severe shock. 3–8 Shi et al. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease.
Jesse McLaren (@ECGcases), of Emergency Medicine Cases Reviewed by Pendell Meyers and Steve Smith An 85yo with a history of hypertension developed chest pain and collapsed, and had bystander CPR. The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology.
Discussion See this post: STEMI with Life-Threatening Hypokalemia and Incessant Torsades de Pointes I could find very little literature on the treatment of severe life-threatening hypokalemia. mEq/L, the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. and/or in the presence of acute MI. mEq/L to 3.0 mEq/L to 2.0
Data that do not establish neurological risk stratification in the first 6 hours after CA include the patient’s age, duration of CPR, seizure activity, serum lactate level or pH, Glasgow motor subscore in patients who received NMB or sedation, pupillary function in patients who received atropine, and optic nerve sheath diameter (95.3%, 20/21).
the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 I could find very little literature on the treatment of severe life-threatening hypokalemia. The estimated deficit associated with a serum decrease from 4.0 If the patient is at 1.8,
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content