This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Date: August 30, 2023 Reference: Griffey et al. Date: August 30, 2023 Reference: Griffey et al. The patient states he has had multiple “diabetic emergencies” in the past and usually ends up in the intensive care unit (ICU) on a drip. He is wondering, “Hey doc, do I have to go back to the ICU strapped to an IV pole?”
Date: June 12th, 2022 Reference: Finfer et al. Balanced Multielectrolyte Solution versus Saline in Critically Ill Adults. Guest Skeptic: Dr. Aaron Skolnik is an Assistant Professor of Emergency Medicine at the Mayo Clinic Alix School of Medicine and Consultant in the Department of CriticalCare Medicine at Mayo Clinic Arizona.
The reality of ever increasing ED volumes and longer boarding times to the ICU makes it imperative for emergency physicians to learn how to manage these critical patients. It was found that patients exposed to deep sedation in the ED had an independent higher incidence of continued deep sedation on ICU day one ( Fuller, 2019 ).
[display_podcast] Date: November 11th, 2017 Reference: Sundén-Cullberg et al. Fever in the Emergency Department Predicts Survival of Patients With Severe Sepsis and Septic Shock Admitted to the ICU. CriticalCare Medicine 2017. display_podcast] Date: November 11th, 2017 Reference: Sundén-Cullberg et al.
Thats exactly what Shane George et al. set out to explore in the Kids THRIVE study investigating whether NHF apnoeic oxygenation could improve intubation outcomes in critically unwell children needing emergency airway management. George S, Williams T, Humphreys S, et al. Lancet Respiratory Medicine.
Date: September 11th, 2019 Reference: Putzu et al. The Effect of Vitamin C on Clinical Outcome in Critically Ill Patients: A Systematic Review with Meta-Analysis of Randomized Controlled Trials. CriticalCare Medicine. Date: September 11th, 2019 Reference: Putzu et al. CriticalCare Medicine.
Paper: Dequin P, Meziani F, Quenot J, et al. ClinicalTrials.gov: NCT02517489 7 Clinical Question: In adult patients with severe community-acquired pneumonia admitted to the ICU, does early hydrocortisone treatment, compared to standard therapy, reduce mortality at 28 days? Patients enrolled from 31 Intensive Care Units in France.
Disposition to ICU. References: Yuan TH, Kerns WP, Tomaszewski CA, et al. von Lewinski D, Bruns S, Walther S, et al. Cole JB, Corcoran JN, Engebretsen KM, et al. Holger JS, Engebretsen KM, Fritzlar SJ, et al. Kerns W, Schroeder D, Williams C, et al. Kline JA, Tomaszewski CA, Schroeder JD, et al.
Author: Brit Long, MD (@long_brit) // Reviewed by Alex Koyfman, MD (@EMHighAK) The American Heart Association (AHA) and Neurocritical Care Society (NCS) released their 2023 Scientific Statement on the criticalcare management of post ROSC patients. Statements: Initiate EN as soon as possible after ICU admission (100%, 20/20).
Welcome back to the tasty morsels of criticalcare podcast. This segues relatively nicely into a section of the document on palliative care. It is important to realise that a referral to ICU for refractory cardiorenal syndrome may simply be a sign that the patient is reaching end of life. – Mullens, W.,
Date: September 28th, 2021 Reference: Zampieri et al. Saline Solution on Mortality in Critically Ill Patients: The BaSICS Randomized Clinical Trial. Date: September 28th, 2021 Reference: Zampieri et al. Saline Solution on Mortality in Critically Ill Patients: The BaSICS Randomized Clinical Trial.
Reference: Cashen K, Reeder RW, Ahmed T, et al. Sodium bicarbonate use during pediatric cardiopulmonary resuscitation: a secondary analysis of the icu-resuscitation project trial. Pediatric Crit Care Med. Reference: Cashen K, Reeder RW, Ahmed T, et al. Pediatric Crit Care Med.
Welcome back to the tasty morsels of criticalcare podcast. Vasopressin has some animal data suggesting it causes less rise in PVR than our beloved noradrenaline but take that with an appropriately loosely defined portion of salt given that animal data is not ICU patients. Care 11 , 77–83 (2022). Johnson, S. Barnett, C.
Reference: Peters MJ, et al. Conservative versus liberal oxygenation targets in critically ill children (Oxy-picu): a UK multicentre, open, parallel-group, randomised clinical trial. Clinical Question: What is the optimal target for systematic oxygen in critically ill children receiving invasive ventilation?
Welcome back to the tasty morsels of criticalcare podcast. The major barrier to implementation in the ICU setting is the almost complete absence of ICU patients from these trial cohorts. Welcome back to the tasty morsels of criticalcare podcast. Many penumonias will develope a parapneumonic effusion.
Intensive Care Med 2021 Guest Skeptic: Missy Carter, former City of Bremerton Firefighter/Paramedic, currently a professor of Emergency Medical Services at Tacoma Community College’s paramedic program. Date: January 16th, 2022 Reference: Matchett, G. Etomidate versus ketamine for emergency endotracheal intubation: a randomized clinical trial.
Date: July 16th, 2022 Reference: Lamontagne F et al. Intravenous Vitamin C in Adults with Sepsis in the Intensive Care Unit. Date: July 16th, 2022 Reference: Lamontagne F et al. Intravenous Vitamin C in Adults with Sepsis in the Intensive Care Unit. She is admitted to the intensive care unit (ICU) for septic shock.
Welcome back to the tasty morsels of criticalcare podcast. We’re much less likely to see this cohort in the criticalcare side of things. A follow up trial in 2011 by ICU steroid guru Djilalli Annane did not find a benefit. Intensive Care Medicine 37 , 486–492 (2011). How does it make people sick?
Paper: Haber, EN et al. Accuracy of Noninvasive Blood Pressure Monitoring in Critically Ill Adults. J Intensive Care Med 2024. PMID: 38215002 Clinical Question: In critically ill adults in the ICU is noninvasive blood pressure (NIBP) monitoring similar (≤10% difference) to invasive arterial blood pressure (IABP) monitoring?
Welcome back to the tasty morsels of criticalcare podcast. First up is the VASST trial, (Russel et al 2008 NEJM). Enrolled 800 fairly typical ICU patients, and found a 35% vs 39% mortality benefit favouring the vaso but of course this was below the somewhat arbitrary statistical significance. Gordon, A. Nagendran, M.
3, 4 It is the most common nosocomial infection in patients on mechanical ventilation, and one of the leading causes of nosocomial infection among all patients in the ICU. The low incidence could be a result of the systematic implementation of bundles known to decrease VAP incidence in the ICU. 4, 8 Paper: Dahyot-Fizelier, C.,
Welcome back to the tasty morsels of criticalcare podcast. The incidence of dynamic LVOTO in those with septic shock is remarkably high and is reported to be 20% in one study from ICU echo guru Michel Slama. References Chapter 13, Oxford Textbook of Advanced CriticalCare Echocardiography covers this nicely.
Kapoor et al. 2018) “Sacred Pause Imitative in the ICU: A survey of ICU physicians and nurses”. CriticalCare Medicine , 46 (1), pp. Southern Medical Journal. 112 (9),pp. Newell, J. & & MacNeil, G. 2012) “Professional burnout, vicarious trauma, secondary traumatic stress, and compassion fatigue”.
Secondary Outcomes: Delayed hypotension, increased ICU stay, and other relevant outcomes. 4 studies remained, with a total of 571 patients with sepsis and a history of CHF Critical Result: The weighted OR for death was significantly higher in the <30 × 3 vs. 30 × 3 OR = 1.81, 95% CI = 1.13–2.89, 2.89, p = 0.01.
Welcome back to the tasty morsels of criticalcare podcast. Read More » Welcome back to the tasty morsels of criticalcare podcast. It is critical to understand that this is a test useful in follow up to confirm diagnosis and should not be involved in the decision whether or not to give adrenaline acutely.
This trial aimed to assess whether targeted therapeutic mild hypercapnia (TTMH) applied during the initial 24 hours of mechanical ventilation in the ICU can enhance neurological outcomes at the 6-month mark, as compared to standard care, which involves targeted normocapnia (TN). Paper: Eastwood G, et al. N Engl J Med.
The authors of this study sought to test the hypothesis that intravenous amino acid therapy would lead to a lower occurrence of postoperative AKI when compared to placebo. Paper: Landoni G. Intravenous amino acid therapy for kidney protection in cardiac surgery a protocol for a multi-centre randomized blinded placebo controlled clinical trial.
Treatment is supportive with respiratory therapy, criticalcare, inotropic therapy, and cardiac life support. If AFE occurs during labor, immediate delivery is recommended. ” Obstet Gynecol 123(2 Pt 1): 337-348. link] Society for Maternal-Fetal Medicine. Electronic address, p. ” Am J Obstet Gynecol 215(2): B16-24.
Paper: Singer S, et al. The safety and efficacy of push dose vasopressors in critically ill adults. References: Singer S, et al. The safety and efficacy of push dose vasopressors in critically ill adults. PMID: 36108346 Cole JB, et al. PMID: 31270748 Maheshwari K, et al. Intensive Care Med.
ICU time and ED time are different. In the ICU, we have a useful (albeit sometimes flexible) cap: our total number of beds.* References Patel KK, Young L, Howell EH, et al. This differs from the main questions of many of their consulting and admitting specialties.* Remember that nobody sees anyone else’s denominator.
100% seems too good to be true Morello et al., Clin Exp Allergy. 2024 Oct 9. doi: 10.1111/cea.14565. Epub ahead of print. PMID: 39383344 Profundus Trial – Can we actually exclude acute aortic syndromes with this protocol? Diagnosis of acute aortic syndromes with ultrasound and D-dimer: the PROFUNDUS study.
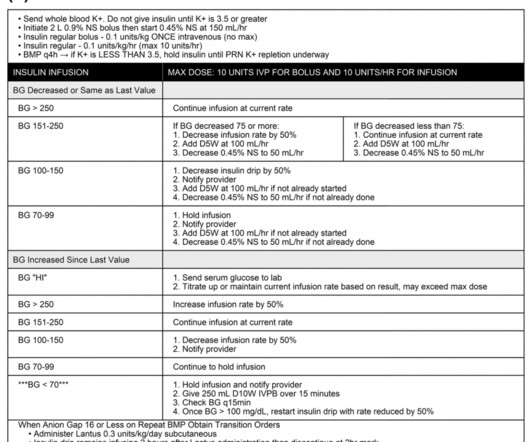
Intravenous insulin infusions typically require treatment in highly monitored settings, such as an intensive care unit (ICU) or step-down unit for safety and due to the frequency and intensity of monitoring. ICU and step-down beds are a limited resource and generate higher hospital charges. Diabetes Care. Diabetes Care.
2 Finally the settings initiated early in a patient’s care are often carried forward unchanged into their hospital and ICU stay. The result of this ED capacity strain and less than ideal patient to staff ratios has led to delays in interventions, treatments and care adjustments. Paper: Owyang CG, et al. J Crit Care.
The Importance of Civility in CriticalCare Resuscitation A 3-year-old patient with diabetic ketoacidosis arrives at your ED. The team sits down for a hot debrief once the patient is stabilised and transferred to the ICU. Conclusion Criticalcare resuscitation is stressful. Incivility can mean many things.
4 With the increasing utilization of EEG, especially continuous EEG, nonconvulsive seizures have been increasingly recognized and diagnosed as a cause of altered mental status in critically ill patients. Neurology consultation should be initiated, and the patient should be admitted to the ICU. Towne AR, Waterhouse EJ, Boggs JG, et al.
Ketamine vs etomidate in ICU intubation ? The PEACH trial: No body had a fit, so… we have no clue Peter-Derex L, Philippeau F, Garnier P, et al. PMID: 30206143 Less is more when it comes to intravenous fluids de-Madaria E, Buxbaum JL, Maisonneuve P, et al. Anaesth Crit Care Pain Med. 2018 Sep 11;362:k3843.
Louis) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) Case You are working in the trauma/criticalcare pod of your emergency department (ED). He requires low-dose epinephrine to maintain his mean arterial pressure (MAP) in the 60s mmHg and is transported to the cardiothoracic (CT) ICU. Carsten L, et al.
4 Prompt consultation is imperative with thoracic surgery, interventional radiology (IR), gastroenterology (GI), and/or criticalcare. Disposition : Admission to ICU with potential GI, IR, and/or surgical management. In: Tintinalli JE, Ma OJ, Yealy DM, et al., Discuss with GI/surgeons prior to placement.
Current practice is still isotonic fluids with a slight volume restriction, but there may/may not be another fluid shift coming… References Alobaidi R, Basu RK, Decaen A, et al. Fluid Accumulation in Critically Ill Children. Crit Care Med. Ann Intensive Care. doi:10.1186/s13613-018-0402-x McNab S, Duke T, South M, et al.
You contact ICU, anaesthetics, ENT, and oncology with a plan to attempt more definitive imaging in the prone position (which Ginny tells you is much comfier) What’s the evidence for our emergent management? 0000000000000294 Carter BW, Benveniste MF, Madan R, et al. A CXR demonstrates a mediastinal mass. J Thorac Oncol.
Article: de-Madaria E et al. For More on This Topic Checkout: CorePendium: Pancreatic Disease Internet Book of CriticalCare: Acute Pancreatitis EMCrit: Ep333 – The State of Fluids Show with the EMCrit Core Team The Bottom Line: Aggressive or Moderate Fluid Resuscitation in Acute Pancreatitis References: de-Madaria E et al.
Nielsen N, Wetterslev J, Cronberg T et al. By the time of the study by Nielsen et al. However, the decade since the original Hypothermia after Cardiac Arrest trial had seen significant advances in pre-hospital, emergency department, and criticalcare that may have contributed to these outcomes. Kirkegaard et al.
Recent studies on patients requiring criticalcare have demonstrated that hyperoxia is harmful and instead we should be targeting normoxia (SpO2>93%). Paper 1: Schmidt HJ et al. PMID: 360027567 [ Access on Read by QxMD ] Paper 2: Kjaergaard J et al. References: Schmidt HJ et al. Liberal O2: 33.9%
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content