This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Reference: Snyder BD, Van Dyke MR, Walker RG, et al. Reference: Snyder BD, Van Dyke MR, Walker RG, et al. You continue with compressions and defibrillations and your partner places an advanced airway. Association of small adult ventilation bags with return of spontaneous circulation in out of hospital cardiac arrest.
St.Emlyn's - Emergency Medicine #FOAMed Should we use AP or AL pad position first for defibrillation in VF/VT cardiac arrest. FOAMed @stemlyns The post JC: AP or AL pad position for first choice shock in VF? appeared first on St.Emlyn's.
Date: February 7, 2023 Reference: Cheskes et al. Defibrillation Strategies for Refractory Ventricular Fibrillation. Date: February 7, 2023 Reference: Cheskes et al. Defibrillation Strategies for Refractory Ventricular Fibrillation. Reference: Cheskes et al. An anesthetist is working with him for the procedures.
Reference: Tanner et al, A retrospective comparison of upper and lower extremity intraosseous access during out-of-hospital cardiac arrest resuscitation. Reference: Tanner et al, A retrospective comparison of upper and lower extremity intraosseous access during out-of-hospital cardiac arrest resuscitation. Prehospital Emergency Care.
Date: July 21, 2023 Reference: Prekker et al. Date: July 21, 2023 Reference: Prekker et al. We should focus more on high-quality CPR and early defibrillation for shockable rhythms and less on type of supraglottic airway device. Video versus Direct Laryngoscopy for Tracheal Intubation of Critically Ill Adults.
2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. Initial guidelines defined “refractory” as VT or VF occurring despite three shocks from a cardiac defibrillator. Tips for use of dual sequence defibrillation 11 : Use the same model of defibrillator.
Date: December 6th , 2018 Reference: Perkins et al. Date: December 6th , 2018 Reference: Perkins et al. A cardiac defibrillator is hooked up and the patient is in ventricular fibrillation. JAMA 2009, Hagihara et al. JAMA 2012 and Cournoyer et al. A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest.
Reference: Derkenne et al. Reference: Derkenne et al. You abandon your coffee order and quickly head next-door, where you are able to start cardiopulmonary resuscitation (CPR) and direct a bystander to find the store’s automated external defibrillator (AED) while waiting for emergency medical services (EMS) to arrive.
Multiple attempts at defibrillation, epinephrine, and amiodarone have been unsuccessful. Problem What is the best defibrillation strategy to treat refractory ventricular fibrillation? 2,3 Multiple published studies have addressed treatment of ventricular fibrillation with defibrillation and medications such as amiodarone and lidocaine.
Date: October 18th, 2022 Reference: Moore et al. Date: October 18th, 2022 Reference: Moore et al. This includes epinephrine for OHCA, target temperature management, mechanical CPR, supraglottic airways, steroids, hands on defibrillation and many more topics. first appeared on The Skeptics Guide to Emergency Medicine.
[display_podcast] Date: September 19th, 2017 Reference: Cournoyer et al. display_podcast] Date: September 19th, 2017 Reference: Cournoyer et al. Bystander high-quality CPR can buy you some time until defibrillation. We know that rapid application of electricity to defibrillate shockable arrhythmias save lives.
Background Information: Double external defibrillation (DED) is an intervention often used to treat refractory ventricular fibrillation (RVF). This procedure involves applying another set of pads attached to a second defibrillator to a patient and shocking them in hopes of terminating the rhythm. N Engl J Med.
Date: March 8, 2023 Reference: Smida et al. Date: March 8, 2023 Reference: Smida et al. A fire company is on scene providing high-quality cardiopulmonary resuscitation (CPR) and has defibrillated twice with an automated external defibrillator (AED). Reference: Smida et al.
St.Emlyn's - Emergency Medicine #FOAMed Should we use AP or AL pad position first for defibrillation in VF/VT cardiac arrest. FOAMed @stemlyns The post AP or AL pad position for first choice shock in VF? appeared first on St.Emlyn's.
[display_podcast] Date: September 21st, 2018 Reference: Kawano et al. display_podcast] Date: September 21st, 2018 Reference: Kawano et al. One defibrillation for ventricular fibrillation (VF) is provided but the patient remains in VF. Case: A 46-year-old man has a cardiac arrest at home, witnessed by family.
3: Does Defibrillator Pad Placement Matter for OHCA? Source Initial Defibrillator Pad Position and Outcomes for Shockable Out-of-Hospital Cardiac Arrest. Source Emergency Department Blood Pressure Treatment and Outcomes in Adults Presenting with Severe Hypertension. West J Emerg Med. 2024;25(5):680-689. #3: JAMA Netw Open. 2024.31673.
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). The TOMAHAWK Investigators. first appeared on The Skeptics Guide to Emergency Medicine.
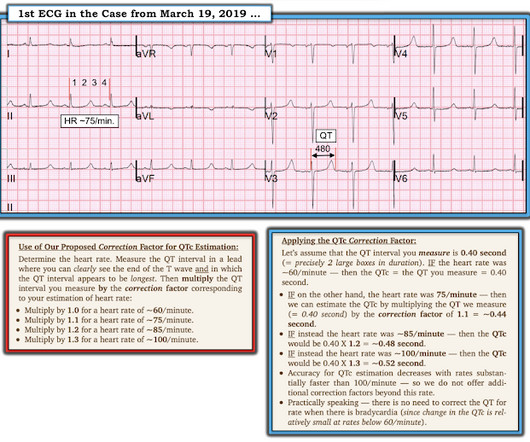
Bogossian et al. (1) Bogossian H, Frommeyer G, Ninios I, Hasan F, Nguyen QS, Karosiene Z, Mijic D, Kloppe A, Suleiman H, Bandorski D, et al. So the best way to measure whether there is prolongation within an individual is to measure changes in either the JT interval or the T-peak to T-end interval (1, 2). Heart Rhythm [Internet].
Date: January 5th, 2021 Reference: Grunau et al. Date: January 5th, 2021 Reference: Grunau et al. Reference: Grunau et al. OHCA was defined as persons found apneic and without a pulse who underwent either external defibrillation (bystanders or EMS) or chest compressions.
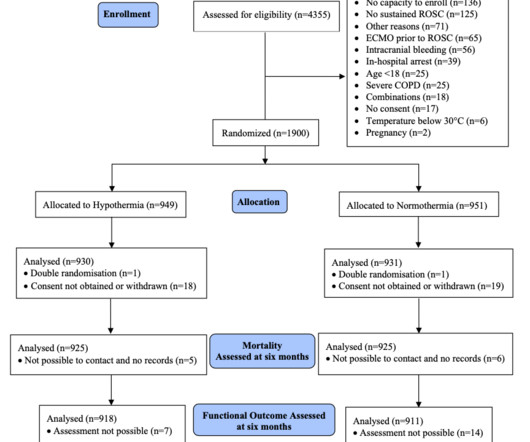
Reference: Dankiewicz et al: TTM2 Trial Investigators. Reference: Dankiewicz et al: TTM2 Trial Investigators. Paramedics managed to get return of spontaneous circulation after a single defibrillation, but the patient is still comatose on arrival. Hypothermia versus Normothermia after Out-of-Hospital Cardiac Arrest.
Reference: Cashen K, Reeder RW, Ahmed T, et al. Reference: Cashen K, Reeder RW, Ahmed T, et al. Apart from high-quality CPR and early defibrillation, many other interventions we try lack a strong evidence base. Pediatric Crit Care Med. Pediatric Crit Care Med.
1 Like other implantable devices, such as pacemakers and automated implantable cardioverter defibrillators (AICDs), they can be interrogated for valuable information by the patient ’ s cardiology team when the patient presents to the ED. Angermann CE, Assmus B, Anker SD, et al. Brugts JJ, Radhoe SP, Clephas PRD, et al.
He underwent further standard resuscitation EXCEPT that we applied the Inspiratory Threshold Device ( ResQPod ) AND applied Dual Sequential Defibrillation (this simply means we applied 2 sets of pads, had 2 defib machines, and defibrillated with both with only a fraction of one second separating each defibrillation.
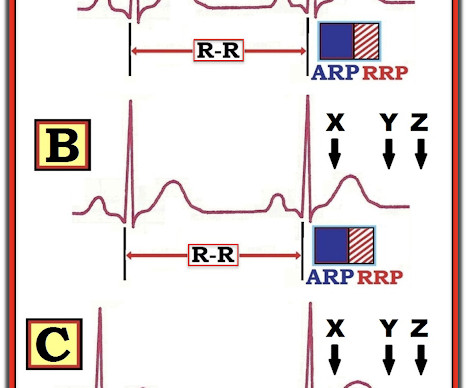
We can, therefore, put down the defibrillation pads, set aside the amiodarone, and look further at the ECG. Paradoxically, though, the third green arrow identifies a QRS that is more narrow than the RBBB complexes surrounding it. Question 2: What explains the conduction abnormalities? References Chiale, P. JACC, Vol 23, No 3; 724-32.
After the fourth defibrillation attempt, 200 mcg IV NTG was administered, resulting in immediate return of spontaneous circulation with a junctional bradycardia rhythm. References Prinzmetal M, Kennamer R, Merliss R, et al. Myerburg RJ, Kessler KM, Mallon SM et al. Magid DJ, Aziz K, Cheng A, et al. Click to enlarge.)
Two hours later , the patient returned to this same urgent care facility with worsening chest pain, and this ECG was performed: While getting another ECG, the patient suffered cardiac arrest: After multiple defibrillations, ROSC was achieved with ongoing "STEMI". Most OMI have a peak Troponin T over 1000 ng/L [reference: Baro R et al.
Defibrillator pads are placed and you give 2 g IV magnesium over ten minutes. Figure 3/ Adapted from Wilde et al. A complete approach to treating cLQTS can be found in Wilde et al 2. It is recommended to use an unsynchronized setting as the defibrillator may not be able to track the R-wave in the polymorphic waveform.
Patients with a history of life-threatening or recurrent VT will often undergo radiofrequency catheter ablation and/or placement of a cardioverter defibrillator (implantable or external). Reference Anjeza Cipi MD, et al. See the original question here.) Member Benefit: All ACEP members receive a 20 percent discount on VisualDX.
The PEACH trial: No body had a fit, so… we have no clue Peter-Derex L, Philippeau F, Garnier P, et al. PMID: 30206143 Less is more when it comes to intravenous fluids de-Madaria E, Buxbaum JL, Maisonneuve P, et al. PMID: 35490863 Hands on defibrillation: Even if it’s safe, would it actually help? N Engl J Med.
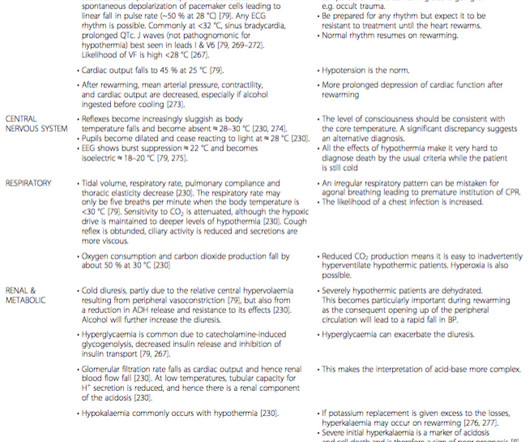
ERC 2015 guidelines recommend withholding adrenaline administration in hypothermic CA (HT IV) and limiting defibrillation to three attempts until the core temperature is >30 °C. The benefit of antiarrhythmic drugs in hypothermic CA is unclear.
CPR is taken over by responding crews, and he is placed on a cardiac monitor/defibrillator. After several cycles of defibrillation, epinephrine, and amiodarone, the patient remains in cardiac arrest. Current AHA guidelines do not recommend routine use of calcium in cardiac arrest (Panchal, et al.,
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She was immediately intubated during continued compressions, then underwent a 9th defibrillation, which resulted in an organized rhythm at 42 minutes after initial arrest. see below).
Background: There are only two interventions that have been proven in the medical literature to improved outcomes in cardiac arrest: high-quality CPR and early defibrillation. Article: Moore JC et al. References: Moore JC et al. It is imperative that we continue to look at ways to improve cardiac arrest resuscitation.
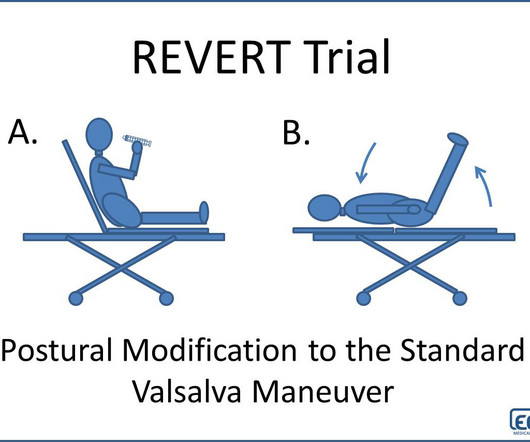
Additional Treatments Defibrillation pads were applied. References Appelboam A, Reuben A, Mann C et al. Baker A, Whitbread M, Richmond L et al. Unfortunately, in this case the maneuver was attempted twice without success. IV access was achieved. The heart rhythm converts to sinus tachycardia. The Lancet.
Here, we present them in alphabetical order: ABC – Airway, Breathing and Circulation – “This is the Golden Rule of emergency medical professionals” AED – Automated External Defibrillator – The device that delivers electric shock to the heart of patients experiencing sudden cardiac arrest A-EMT – Advanced EMT ALS – Advanced Life Support Anaphylaxis— (..)
After resuscitation and defibrillation , there were no more episodes of TdP. Below is the patient’s 12 lead ECG following defibrillation. Most Torsades is the result of a pause-dependent effect that predisposes to development of the malignant arrhythmia ( Dohadwala et al — Heart Rhythm Case Rep 3(2):115-119, 2017 ).
Meyers et al. Aslanger et al. Lemkes et al. Bergmark et al. There was 100% proximal LAD occlusion, EF was 55% with severe hypokinesis to mid-distal septum and apex. First troponin I was 150 ng/L (normal <26 in males and <16 in females) and peak was 7,500. Int J Cardiol Heart Vasc 2021 2. Eur Heart J 2018 4.
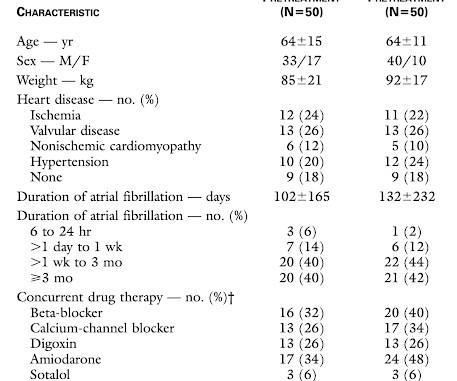
We examined the effect of ibutilide, a class III antiarrhythmic agent, on the energy requirement for atrial defibrillation and assessed the value of this agent in facilitating cardioversion in patients with atrial fibrillation that is resistant to conventional transthoracic cardioversion.
She was defibrillated and resuscitated. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Lindahl et al. From Gue at al. Lindahl B, Baron T, Erlinge D, et al. Upon arrival to the emergency department, a senior emergency physician looked at the ECG and said "Nothing too exciting."
the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. Here are other posts on hyperK, large calcium doses for hyperK, and ventricular tachycardia in hyperK Weakness, prolonged PR interval, wide complex, ventricular tachycardia Very Wide and Very Fast, What is it? How would you treat? Medicine (Baltimore) 1981;60:339-54].
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. Lemkes JS, Janssens GN, van der Hoeven NW, et al. We at Hennepin recently published this study Sharma et al. Figure-1: I've labeled the initial ECG in today's case ( recorded after successful defibrillation ). 5% vs. 58%!!
As this case shows, electrical capture isn't always possible at lower currents, especially with pads placed in a standard anterolateral "defibrillation" position. The University of Maryland found that capture occurred in only 42-78% of patients, dependent on pad positioning (Moayedi et al, 2022).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content