This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
After the fourth defibrillation attempt, 200 mcg IV NTG was administered, resulting in immediate return of spontaneous circulation with a junctional bradycardia rhythm. Cardiac arrest secondary to myocardial ischemia from coronary vasospasm is well documented. References Prinzmetal M, Kennamer R, Merliss R, et al. N Engl J Med.
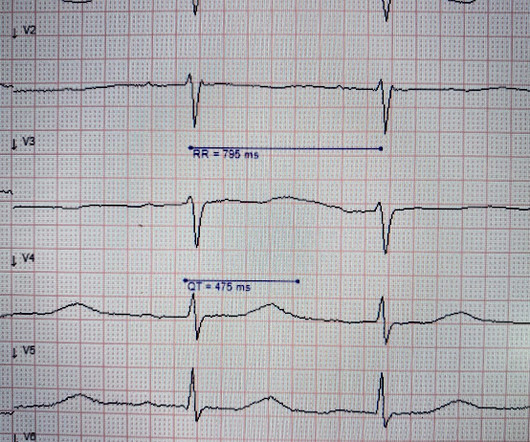
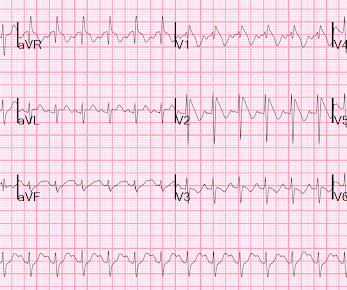
He required multiple defibrillations within a period of a few hours. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. In both tracings — an exceedingly fast PMVT is documented. Below are printouts of some of the arrhythmias recorded. What do you think?
Brugada sign refers to the findings on ECG, while Brugada syndrome is the combination of ECG findings with one of the following: documented ventricular tachycardia or fibrillation, syncope, family history of sudden cardiac death at < 45 years old, or inducible ventricular tachycardia with programmed electrical stimulation. Circulation.
Defibrillator pads are placed and you give 2 g IV magnesium over ten minutes. Figure 3/ Adapted from Wilde et al. A complete approach to treating cLQTS can be found in Wilde et al 2. It is recommended to use an unsynchronized setting as the defibrillator may not be able to track the R-wave in the polymorphic waveform.
This episode self terminated before defibrillation was possible. See Costagliola et al — Ann Clin Transl Neurol 8(7): 1557-1568, 2021 — for more on the complex "Brain-Heart Interaction" in Epilepsy ). This run of TdP is initiated by a PVC — but it then self-terminates. Discussion : The patient in today’s case presented with "seizures".
Stredder et al, Archives of Disease in Childhood 2016 we see that 58% were not asked about triggers, 30% were not asked about duration and, importantly for risk stratification, 59% were not asked for a family history of cardiac disease. Where there are a number of unexplained deaths, start to be more critical about what this could mean.
Our patient had a Brugada Type 1 pattern elicited by an elevated core temperature, which is also a documented phenomenon. In the largest study looking at this topic by Mizusawa et al., Recently the rate of true arrhythmic events related to fevers in the classic Brugada Type 1 syndrome was explored by Michowitz et al.
At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia." However it is classified is not so important!
Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia." the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. How would you treat? If cardiac arrest from hypokalemia is imminent (i.e., Give an initial infusion of 10 mEq IV over 5 minutes; repeat once if needed.
I B ECG monitoring should start immediately and a defibrillator must be ready. I C Cardioversion In patients with documented de novo AF during the acute phase of STEMI, long-term oral anticoagulation should be considered depending on CHA2DS2-VASc score and taking concomitant antithrombotic therapy into account.
Thus, Brugada is the likely diagnosis _ A very nice explanation of this is given in the document quoted below on current ECG criteria for Brugada pattern. Bayes de Luna, A et al. This is based on the Sieira et al, 2017, risk calculator , which gives a borderline risk score (2). J Electrocardiology 45 (2012):433-442.
Documentation indicates that the patient was shocked 4 times (with no comment on energy level) and received amiodarone 300 mg IV and magnesium 2 g IV. In this case, you should get a second defibrillator and perform double sequential external defibrillation (DSED). In fact, in this elegant study by Heitner et al.
He was defibrillated twice and received two doses of epinephrine, with return of spontaneous circulation. A repeat ECG (see figure 3) was performed utilizing the technique described by Sangwatanaroj et al., He underwent placement of a dual chamber, implantable, cardioverter-defibrillator (ICD) placement on hospital day 5.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content