This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Reference: Tanner et al, A retrospective comparison of upper and lower extremity intraosseous access during out-of-hospital cardiac arrest resuscitation. Reference: Tanner et al, A retrospective comparison of upper and lower extremity intraosseous access during out-of-hospital cardiac arrest resuscitation. Prehospital Emergency Care.
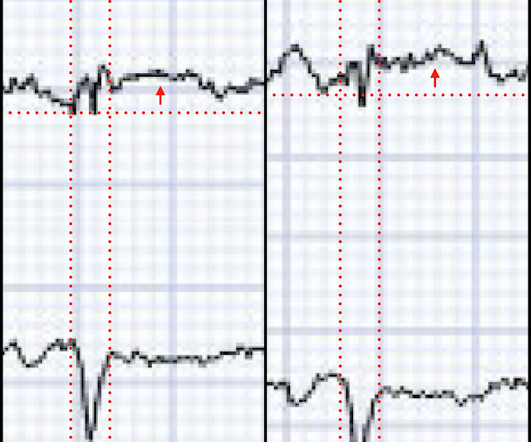
On ED arrival ROSC is achieved. As this case shows, electrical capture isn't always possible at lower currents, especially with pads placed in a standard anterolateral "defibrillation" position. The University of Maryland found that capture occurred in only 42-78% of patients, dependent on pad positioning (Moayedi et al, 2022).
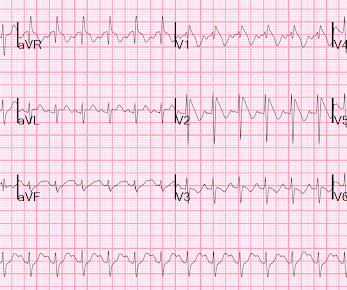
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. Here was his initial ED ECG: Formal interpretation by interventional cardiologist: There is "Non-diagnostic" ST Elevation in V2-V4 and aVL. Lemkes JS, Janssens GN, van der Hoeven NW, et al. 5% vs. 58%!!
emergency departments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. 2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. Tips for use of dual sequence defibrillation 11 : Use the same model of defibrillator.
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP).
Date: January 5th, 2021 Reference: Grunau et al. Date: January 5th, 2021 Reference: Grunau et al. Case: During a busy emergency department (ED) shift the paramedic phone rings. Reference: Grunau et al. first appeared on The Skeptics Guide to Emergency Medicine.
Reference: Cashen K, Reeder RW, Ahmed T, et al. Reference: Cashen K, Reeder RW, Ahmed T, et al. Case: A 6-month-old boy presents to the emergency department (ED) with three days of worsening cough, cold symptoms, and fever. Background: We often manage patients in cardiac arrest in the ED or the intensive care unit (ICU).
Louis) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) Case You are working in the trauma/critical care pod of your emergency department (ED). His blood sugar was normal en route to the ED, and his initial rhythm on the cardiac monitor was asystole. It is unclear how long he was down.
We can, therefore, put down the defibrillation pads, set aside the amiodarone, and look further at the ECG. Chou’s Electrocardiography in Clinical Practice (6th ed). Paradoxically, though, the third green arrow identifies a QRS that is more narrow than the RBBB complexes surrounding it. References Chiale, P. JACC, Vol 23, No 3; 724-32.
After the fourth defibrillation attempt, 200 mcg IV NTG was administered, resulting in immediate return of spontaneous circulation with a junctional bradycardia rhythm. Dr. Rad is ED faculty at Wellstar Kennestone Regional Medical Center in Marietta, Ga., References Prinzmetal M, Kennamer R, Merliss R, et al. Click to enlarge.)
A 40-something with persistent Ventricular Fibrillation presented after attempted prehospital resuscitation A 40-something with no previous cardiac history presented to the ED in persistent Ventricular Fibrillation after attempted prehospital resuscitation. Finally, head-up CPR (which was not used here), makes for better resuscitation.
In this medical system, the EMS provider can then be routed to the ED or to a type of urgent care facility that is open 24 hrs/day and staffed by a primary care provider. Most OMI have a peak Troponin T over 1000 ng/L [reference: Baro R et al. In this case, the EMS provider was routed to the urgent care facility.
Defibrillator pads are placed and you give 2 g IV magnesium over ten minutes. Figure 3/ Adapted from Wilde et al. A complete approach to treating cLQTS can be found in Wilde et al 2. It is recommended to use an unsynchronized setting as the defibrillator may not be able to track the R-wave in the polymorphic waveform.
A 36-year-old female presents to the ED after experiencing an episode of sudden syncope. Patients with Brugada syndrome should have a prompt cardiology consultation for consideration of implantable defibrillator placement due to the high risk of sudden cardiac death. Priori SG, Napolitano C, Gasparini M, et al. Circulation.
Prioritise listening to the first 30 minutes which given a good overview of aetiology and treatment (53 mins) Basics of cardiac rhythm problems in the ED Palpitations are a common reason for children to present to the emergency department, the majority of these will be benign from a cardiac perspective and instead related to stress or anxiety.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. at the time of the ECG.
Here, we present them in alphabetical order: ABC – Airway, Breathing and Circulation – “This is the Golden Rule of emergency medical professionals” AED – Automated External Defibrillator – The device that delivers electric shock to the heart of patients experiencing sudden cardiac arrest A-EMT – Advanced EMT ALS – Advanced Life Support Anaphylaxis— (..)
She was never seen to be in ventricular fibrillation and was never defibrillated. She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR.
If the patient only had these two ECGs recorded, it would have missed the transient time between them which were STEMI positive, and the patient would then have arrived at the ED as “serial ECGs STEMI negative." Meyers et al. Aslanger et al. Lemkes et al. Bergmark et al. Int J Cardiol Heart Vasc 2021 2.
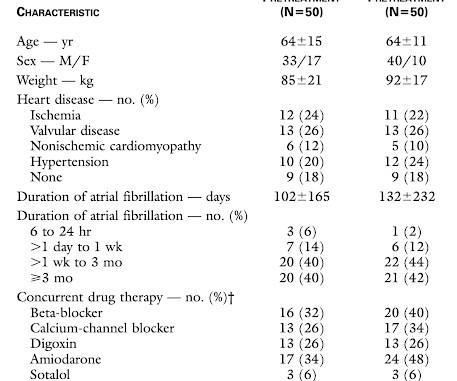
We examined the effect of ibutilide, a class III antiarrhythmic agent, on the energy requirement for atrial defibrillation and assessed the value of this agent in facilitating cardioversion in patients with atrial fibrillation that is resistant to conventional transthoracic cardioversion. Methods. . =
Only 5-18% of ED patients with chest pain have a myocardial infarction of any kind. Cardioversion/defibrillation. Figure-2: TOP: ECG Brugada-1 and Brugada-2 patterns ( from Bayés de Luna et al: J. Could this be a coincidence that the patient was experiencing chest pain and upon ECG capture the atypical brugada pattern was found?
The patient was put on Extracorporeal Life Support in the ED 3 hours after initial resuscitation, the core temp was 30° C and the patient was defibrillated with a single attempt. This Transesophageal ED Echo was recorded: Cardiac POCUS.mov from Stephen Smith on Vimeo. Rituparna et al — as well as Chauhan and Brahma ( Int.
Rhythm B: This patient was seen in the ED — and thought to be in AFlutter with 4:1 AV conduction. Rhythm C: This telemetry strip from an older adult was initially thought to need defibrillation. Rhythm A: This rhythm strip was observed on telemetry — and thought to be AFlutter. The January 30, 2018 post — for PTA.
She was defibrillated and resuscitated. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Lindahl et al. From Gue at al. Lindahl B, Baron T, Erlinge D, et al. Upon arrival to the emergency department, a senior emergency physician looked at the ECG and said "Nothing too exciting."
In the largest study looking at this topic by Mizusawa et al., Recently the rate of true arrhythmic events related to fevers in the classic Brugada Type 1 syndrome was explored by Michowitz et al. 88 patients with fever induced Brugada Type 1 ECG changes without history of syncope or VF/VT were analyzed. There was a 0.9%
They transported to the ED. The history, obtained subsequently, is interesting: The patient had been seen at an outside ED 2 days prior and the K was 2.5 Hospital admission had been recommended, but she left that ED against medical advice. the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al.
Here is his ED ECG: There is obvious infero-posterior STEMI. At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al.
A 67-year-old man presents to the emergency department (ED) in cardiac arrest. Multiple attempts at defibrillation, epinephrine, and amiodarone have been unsuccessful. On ED presentation, he is unresponsive and the monitor shows ventricular fibrillation. He was found by bystanders after he collapsed and 911 was called.
He has been taking increased doses of torsemide without improvement in his symptoms and was directed to the ED for inpatient therapy. Now, a remote outpatient pulmonary arterial pressure monitor and other heart failure detection devices (Table 1) are available that you may begin to see in your ED.
Bayes de Luna, A et al. This is based on the Sieira et al, 2017, risk calculator , which gives a borderline risk score (2). If there are any syncopal or presyncopal events, she should be evaluated immediately in the ED. --All An EP study might be helpful in symptomatic patients (Sroubek et al., Heart Rhythm 2016.
This is what the providers in the ED understood on patient arrival: Patient called 911 for syncope, then had witnessed PEA arrest after medics arrived. She was brought to the ED in a deep coma with GCS of 3, with vital signs, and an ECG was recorded: What do you think? Not a shockable rhythm. including epinephrine, and there was ROSC.
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). The ECG in Figure-1 however, shows no signs of arrhythmogenic cardiomyopathy. See this case for an in-depth discussion of AC and an example of VT and ECG changes associated with this disorder. Van Zyl, M.,
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content