This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Reference: Tanner et al, A retrospective comparison of upper and lower extremity intraosseous access during out-of-hospital cardiac arrest resuscitation. Prehospital Emergency Care. first appeared on The Skeptics Guide to Emergency Medicine. Prehospital Emergency Care. Prehospital Emergency Care. February 2024.
emergencydepartments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. 2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. Out-of-hospital cardiac arrest is a commonly encountered entity in U.S.
Spoon Feed This was a multi-hospital retrospective study of patients who presented to the emergencydepartment with severe hypertension without end organ damage. Source EmergencyDepartment Blood Pressure Treatment and Outcomes in Adults Presenting with Severe Hypertension. West J Emerg Med. 2024;25(5):680-689. #3:
Date: September 8th, 2021 Reference: Desch et al. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. first appeared on The Skeptics Guide to Emergency Medicine. Date: September 8th, 2021 Reference: Desch et al.
Date: February 26th, 2019 Reference: Benger et al. JAMA 2018 Guest Skeptic: Missy Carter, former City of Bremerton Firefighter/Paramedic, currently a physician assistant practicing in emergency medicine in the Seattle area and an adjunct faculty […] The post SGEM#247: Supraglottic Airways Gonna Save You for an OHCA?
Date: January 5th, 2021 Reference: Grunau et al. JAMA 2020 Guest Skeptic: Mike Carter is a former paramedic and current PA practicing in pulmonary and critical care as well as an adjunct professor of emergency medical services […] The post SGEM#314: OHCA – Should you Take ‘em on the Run Baby if you Don’t get ROSC?
Reference: Cashen K, Reeder RW, Ahmed T, et al. Case: A 6-month-old boy presents to […] The post SGEM#394: Say Bye Bye Bicarb for Pediatric In-Hospital Cardiac Arrest first appeared on The Skeptics Guide to Emergency Medicine. Reference: Cashen K, Reeder RW, Ahmed T, et al. Pediatric Crit Care Med. Pediatric Crit Care Med.
Louis) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) Case You are working in the trauma/critical care pod of your emergencydepartment (ED). You receive a page for a cardiac arrest and take report from emergency medical services (EMS). Carsten L, et al. What would your next steps be?
[display_podcast] Date: November 24th, 2017 Reference: Andersen et al. JAMA 2017 Guest Skeptic: Dr. Bob Edmonds is an Emergency Physician in the US Air Force. He is currently deployed, practicing emergency medicine in an undisclosed location. display_podcast] Date: November 24th, 2017 Reference: Andersen et al.
After the fourth defibrillation attempt, 200 mcg IV NTG was administered, resulting in immediate return of spontaneous circulation with a junctional bradycardia rhythm. No existing algorithm or literature guides the validity of a NTG strategy for vasospastic cardiac arrest in the emergencydepartment. Click to enlarge.)
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby EmergencyDepartment where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
A 23-year-old man with no significant medical history presents to the emergencydepartment for evaluation of a syncopal episode. Patients with Brugada syndrome should have a prompt cardiology consultation for consideration of implantable defibrillator placement due to the high risk of sudden cardiac death. Circulation.
Authors: Adam Roussas, MD, MBA, MSE // Reviewed by: Jamie Santistevan, MD ( @jamie_rae_EMdoc, EM Physician, Presbyterian Hospital, Albuquerque, NM); Manpreet Singh, MD ( @MPrizzleER ); and Brit Long, MD ( @long_brit ) Case A 40-year-old female presents to the emergencydepartment for palpitations and lightheadedness.
Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." She was defibrillated and resuscitated. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Lindahl et al. From Gue at al. References: 1.
The PEACH trial: No body had a fit, so… we have no clue Peter-Derex L, Philippeau F, Garnier P, et al. PMID: 30206143 Less is more when it comes to intravenous fluids de-Madaria E, Buxbaum JL, Maisonneuve P, et al. PMID: 35490863 Hands on defibrillation: Even if it’s safe, would it actually help? Emerg Med J.
CPR is taken over by responding crews, and he is placed on a cardiac monitor/defibrillator. After several cycles of defibrillation, epinephrine, and amiodarone, the patient remains in cardiac arrest. Current AHA guidelines do not recommend routine use of calcium in cardiac arrest (Panchal, et al.,
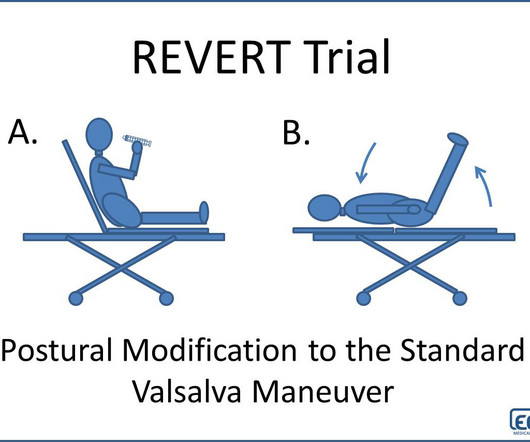
Additional Treatments Defibrillation pads were applied. The patient briefly considered refusing transport to the EmergencyDepartment. References Appelboam A, Reuben A, Mann C et al. Baker A, Whitbread M, Richmond L et al. Unfortunately, in this case the maneuver was attempted twice without success. The Lancet.
Defibrillation Strategies for Refractory Ventricular Fibrillation. Vedantham S, Goldhaber SZ, Julian JA, et al; ATTRACT Trial Investigators. Association of Chest Pain Protocol-Discordant Discharge With Outcomes Among EmergencyDepartment Patients With Modest Elevations of High-Sensitivity Troponin. Am J Emerg Med.
Here, we present them in alphabetical order: ABC – Airway, Breathing and Circulation – “This is the Golden Rule of emergency medical professionals” AED – Automated External Defibrillator – The device that delivers electric shock to the heart of patients experiencing sudden cardiac arrest A-EMT – Advanced EMT ALS – Advanced Life Support Anaphylaxis— (..)
Prioritise listening to the first 30 minutes which given a good overview of aetiology and treatment (53 mins) Basics of cardiac rhythm problems in the ED Palpitations are a common reason for children to present to the emergencydepartment, the majority of these will be benign from a cardiac perspective and instead related to stress or anxiety.
She was never seen to be in ventricular fibrillation and was never defibrillated. Kurkciyan et al. Data collected included demographics, initial rhythm, EKG, emergencydepartment (ED) CT and outcomes. Kurkciyan et al., Medics found her apneic and pulseless, began CPR, and she was found to be in asystole.
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergencydepartment for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. Armstrong et al. What do you think?
Colin is an emergency medicine resident beginning his critical care fellowship in the summer with a strong interest in the role of ECG in critical care and OMI. A patient in their 40s with type 1 diabetes mellitus and hyperlipidemia presented to the emergencydepartment with 5 days of “flu-like” illness. Edits by Willy Frick.
I B ECG monitoring should start immediately and a defibrillator must be ready. I B Patients transferred to PCI centres can bypass the emergencydepartment to undergo primary PCI without delay. STEMI , ST-segment elevation acute myocardial infarction ). due to reciprocal ST-segment depressions in V1, V2, V3).
A 67-year-old man presents to the emergencydepartment (ED) in cardiac arrest. Multiple attempts at defibrillation, epinephrine, and amiodarone have been unsuccessful. Problem What is the best defibrillation strategy to treat refractory ventricular fibrillation? The primary outcome was survival to hospital discharge.
1 Like other implantable devices, such as pacemakers and automated implantable cardioverter defibrillators (AICDs), they can be interrogated for valuable information by the patient ’ s cardiology team when the patient presents to the ED. Angermann CE, Assmus B, Anker SD, et al. Brugts JJ, Radhoe SP, Clephas PRD, et al.
Background Information: Double external defibrillation (DED) is an intervention often used to treat refractory ventricular fibrillation (RVF). This procedure involves applying another set of pads attached to a second defibrillator to a patient and shocking them in hopes of terminating the rhythm. N Engl J Med.
After epinephrine, atropine, and defibrillation x 2, there was a return of pulses. Plummer D et al. EmergencyDepartment Two-Dimensional Echocardiography in the Diagnosis of Nontraumatic Cardiac Rupture. A 65 yo woman had felt ill for 36 hours, had seen her MD but without undergoing a cardiac evaluation.
The following ECG was obtained in the emergencydepartment during active chest pain. This is the shock coil and identifies this device as a defibrillator. CRT-D is cardiac resynchronization therapy with defibrillation capability, like the CXR above. Kaye et al. Canepa-Anson et al. ECG 1 What do you think?
With that being said, the manufacturers say that CPR, medications, Defibrillation, Cardioversion, and Anything you would normally do are OKAY. We still defibrillate ventricular fibrillation just as we would any other patient. A Basic Approach to the LVAD Patient in the EmergencyDepartment. 2017); PMID: 31914051).
He was defibrillated twice and received two doses of epinephrine, with return of spontaneous circulation. Initial echocardiogram (ECG) on arrival (see figure 2) to our emergencydepartment revealed normal sinus rhythm, mild interventricular conduction delay (RSR’), and possible right ventricular hypertrophy. Click to enlarge.)
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

































Let's personalize your content