This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
St.Emlyn's - Emergency Medicine #FOAMed Should we use AP or AL pad position first for defibrillation in VF/VT cardiac arrest. FOAMed @stemlyns The post JC: AP or AL pad position for first choice shock in VF? appeared first on St.Emlyn's.
Reference: Snyder BD, Van Dyke MR, Walker RG, et al. Reference: Snyder BD, Van Dyke MR, Walker RG, et al. You continue with compressions and defibrillations and your partner places an advanced airway. Association of small adult ventilation bags with return of spontaneous circulation in out of hospital cardiac arrest.
Date: February 7, 2023 Reference: Cheskes et al. Defibrillation Strategies for Refractory Ventricular Fibrillation. Date: February 7, 2023 Reference: Cheskes et al. Defibrillation Strategies for Refractory Ventricular Fibrillation. Reference: Cheskes et al. An anesthetist is working with him for the procedures.
2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. Initial guidelines defined “refractory” as VT or VF occurring despite three shocks from a cardiac defibrillator. Tips for use of dual sequence defibrillation 11 : Use the same model of defibrillator.
Reference: Tanner et al, A retrospective comparison of upper and lower extremity intraosseous access during out-of-hospital cardiac arrest resuscitation. Reference: Tanner et al, A retrospective comparison of upper and lower extremity intraosseous access during out-of-hospital cardiac arrest resuscitation. Prehospital Emergency Care.
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. Lemkes JS, Janssens GN, van der Hoeven NW, et al. We at Hennepin recently published this study Sharma et al. link] The COACT trial was fatally flawed (see below). They did not keep a register of patients who were not enrolled.
As this case shows, electrical capture isn't always possible at lower currents, especially with pads placed in a standard anterolateral "defibrillation" position. The University of Maryland found that capture occurred in only 42-78% of patients, dependent on pad positioning (Moayedi et al, 2022).
Date: July 21, 2023 Reference: Prekker et al. Date: July 21, 2023 Reference: Prekker et al. We should focus more on high-quality CPR and early defibrillation for shockable rhythms and less on type of supraglottic airway device. Video versus Direct Laryngoscopy for Tracheal Intubation of Critically Ill Adults.
St.Emlyn's - Emergency Medicine #FOAMed Should we use AP or AL pad position first for defibrillation in VF/VT cardiac arrest. FOAMed @stemlyns The post AP or AL pad position for first choice shock in VF? appeared first on St.Emlyn's.
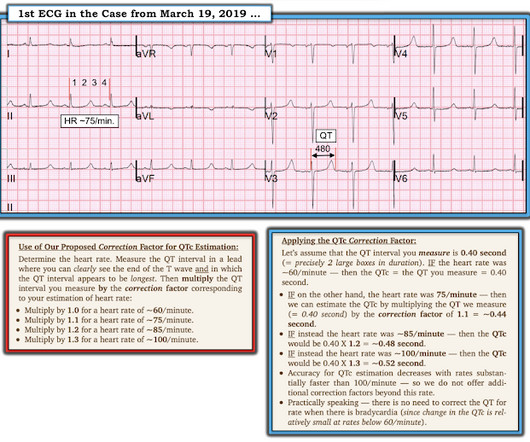
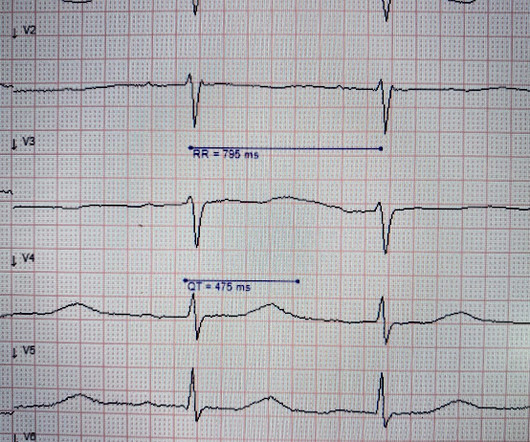
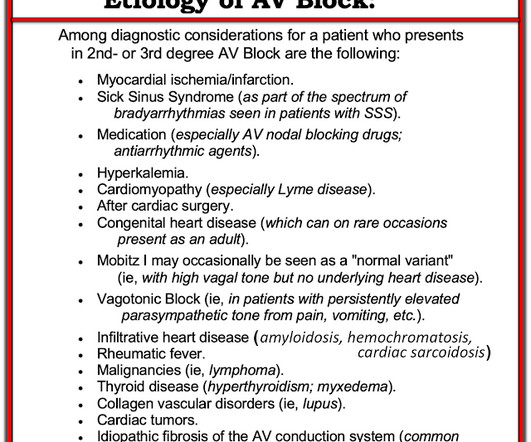
Bogossian et al. (1) Bogossian H, Frommeyer G, Ninios I, Hasan F, Nguyen QS, Karosiene Z, Mijic D, Kloppe A, Suleiman H, Bandorski D, et al. T-waves are quite tall and possibly peaked (HyperK?), but potassium returned normal. What is the QT interval? In LBBB, the QT interval is partly prolonged by the wide QRS. Heart Rhythm [Internet].
Reference: Derkenne et al. Reference: Derkenne et al. You abandon your coffee order and quickly head next-door, where you are able to start cardiopulmonary resuscitation (CPR) and direct a bystander to find the store’s automated external defibrillator (AED) while waiting for emergency medical services (EMS) to arrive.
Date: October 18th, 2022 Reference: Moore et al. Date: October 18th, 2022 Reference: Moore et al. This includes epinephrine for OHCA, target temperature management, mechanical CPR, supraglottic airways, steroids, hands on defibrillation and many more topics. first appeared on The Skeptics Guide to Emergency Medicine.
Date: March 8, 2023 Reference: Smida et al. Date: March 8, 2023 Reference: Smida et al. A fire company is on scene providing high-quality cardiopulmonary resuscitation (CPR) and has defibrillated twice with an automated external defibrillator (AED). Reference: Smida et al.
[display_podcast] Date: September 19th, 2017 Reference: Cournoyer et al. display_podcast] Date: September 19th, 2017 Reference: Cournoyer et al. Bystander high-quality CPR can buy you some time until defibrillation. We know that rapid application of electricity to defibrillate shockable arrhythmias save lives.
Date: December 6th , 2018 Reference: Perkins et al. Date: December 6th , 2018 Reference: Perkins et al. A cardiac defibrillator is hooked up and the patient is in ventricular fibrillation. JAMA 2009, Hagihara et al. JAMA 2012 and Cournoyer et al. A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest.
[display_podcast] Date: September 21st, 2018 Reference: Kawano et al. display_podcast] Date: September 21st, 2018 Reference: Kawano et al. One defibrillation for ventricular fibrillation (VF) is provided but the patient remains in VF. EMS arrives on scene and initiates high quality basic life support (BLS).
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). The TOMAHAWK Investigators. first appeared on The Skeptics Guide to Emergency Medicine.
Date: February 26th, 2019 Reference: Benger et al. Date: February 26th, 2019 Reference: Benger et al. Key to survival is high-quality CPR and early defibrillation. Reference: Benger et al, Effect of a Strategy of a Supraglottic Airway Device vs. Effect of a Strategy of a Supraglottic Airway Device vs.
What is the difference between ALS and BLS Medical Care? In Advanced Life support (ALS) emergencies, a “single” paramedic or ER doctor can not deliver necessary care. And it becomes impossible to treat multi-system injuries, such as doing chest compression (CPR) while trying to open an airway or control bleeding.
3: Does Defibrillator Pad Placement Matter for OHCA? Source Initial Defibrillator Pad Position and Outcomes for Shockable Out-of-Hospital Cardiac Arrest. We always work hard, but we may not have time to read through a bunch of journals. It’s time to learn smarter. West J Emerg Med. 2024;25(5):680-689. #3: JAMA Netw Open. 2024.31673.
Date: January 5th, 2021 Reference: Grunau et al. Date: January 5th, 2021 Reference: Grunau et al. Reference: Grunau et al. OHCA was defined as persons found apneic and without a pulse who underwent either external defibrillation (bystanders or EMS) or chest compressions.
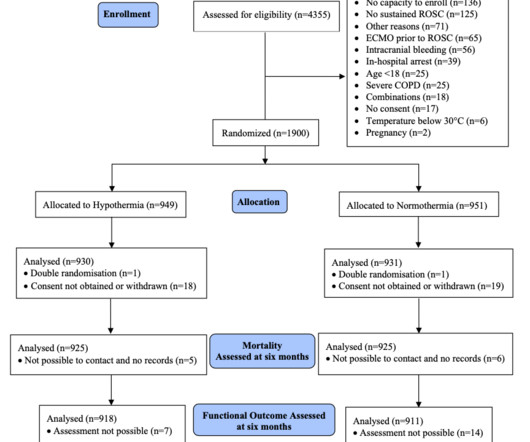
Reference: Dankiewicz et al: TTM2 Trial Investigators. Reference: Dankiewicz et al: TTM2 Trial Investigators. Paramedics managed to get return of spontaneous circulation after a single defibrillation, but the patient is still comatose on arrival. Hypothermia versus Normothermia after Out-of-Hospital Cardiac Arrest.
He required multiple defibrillations within a period of a few hours. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. Some episodes of PMVT would terminate spontaneously — but on many occasions, the PMVT degenerated to VFib, requiring defibrillation.
Reference: Cashen K, Reeder RW, Ahmed T, et al. Reference: Cashen K, Reeder RW, Ahmed T, et al. Apart from high-quality CPR and early defibrillation, many other interventions we try lack a strong evidence base. Pediatric Crit Care Med. Pediatric Crit Care Med. But it’s not that straightforward.
The patient received 1 mg of epinephrine IV x2 with conversion of his rhythm to ventricular fibrillation (VF) for which he was defibrillated twice in the field. The patient is moved over to the stretcher and connected to the monitors and defibrillator. What would your next steps be? His point-of-care labs return with a potassium of 3.4
[display_podcast] Date: November 24th, 2017 Reference: Andersen et al. display_podcast] Date: November 24th, 2017 Reference: Andersen et al. Reference: Andersen et al. Cardiac Arrest: Pulselessness requiring chest compressions and/or defibrillation, with a hospital wide or unit based emergency response.
Article: Branch KHR et al. Known cardiac defibrillator. References: Branch KHR et al. In theory, rapid identification of the underlying cause should improve outcomes by allowing clinicians to tailor management. Advanced imaging post-arrest is a possible modality to achieve this end. Resus 2023. Pre-existing DNR order.
We can, therefore, put down the defibrillation pads, set aside the amiodarone, and look further at the ECG. A 12 Lead ECG was recorded secondary to bizarre telemetry findings at bedside. Said differently, it’s a mess. Paradoxically, though, the third green arrow identifies a QRS that is more narrow than the RBBB complexes surrounding it.
After the fourth defibrillation attempt, 200 mcg IV NTG was administered, resulting in immediate return of spontaneous circulation with a junctional bradycardia rhythm. References Prinzmetal M, Kennamer R, Merliss R, et al. Myerburg RJ, Kessler KM, Mallon SM et al. Magid DJ, Aziz K, Cheng A, et al. Click to enlarge.)
He underwent further standard resuscitation EXCEPT that we applied the Inspiratory Threshold Device ( ResQPod ) AND applied Dual Sequential Defibrillation (this simply means we applied 2 sets of pads, had 2 defib machines, and defibrillated with both with only a fraction of one second separating each defibrillation.
Two hours later , the patient returned to this same urgent care facility with worsening chest pain, and this ECG was performed: While getting another ECG, the patient suffered cardiac arrest: After multiple defibrillations, ROSC was achieved with ongoing "STEMI". Most OMI have a peak Troponin T over 1000 ng/L [reference: Baro R et al.
On arrival, vital signs are stable with a HR of 71, BP of 121/71 mmHg, RR of 17 bpm, and SpO2 of 97% on room air. Physical exam reveals a well-appearing female in no acute distress. Cardiac exam is unremarkable with normal S1/S2 without rubs, gallops or murmurs. Neurological exam is also unremarkable. Her presenting EKG is shown below.
Defibrillator pads are placed and you give 2 g IV magnesium over ten minutes. Figure 3/ Adapted from Wilde et al. A complete approach to treating cLQTS can be found in Wilde et al 2. It is recommended to use an unsynchronized setting as the defibrillator may not be able to track the R-wave in the polymorphic waveform.
This episode self terminated before defibrillation was possible. See Costagliola et al — Ann Clin Transl Neurol 8(7): 1557-1568, 2021 — for more on the complex "Brain-Heart Interaction" in Epilepsy ). This run of TdP is initiated by a PVC — but it then self-terminates. Discussion : The patient in today’s case presented with "seizures".
But artifact is "alive and well" — and learning to recognize it will amaze many of your colleagues ( and may serve to avoid an unnecessary defibrillation or two ). Additional review of ECG artifacts by Pérez-Riera et al ( Ann Noninvasic Electrocardiol 23:e12494, 2018 ) VT Artifact — by Knight et al: NEJM 341:1270-1274, 1999.
Patients with a history of life-threatening or recurrent VT will often undergo radiofrequency catheter ablation and/or placement of a cardioverter defibrillator (implantable or external). Reference Anjeza Cipi MD, et al. Other treatments include electrical cardioversion and the use of antiarrhythmic drugs (e.g.,
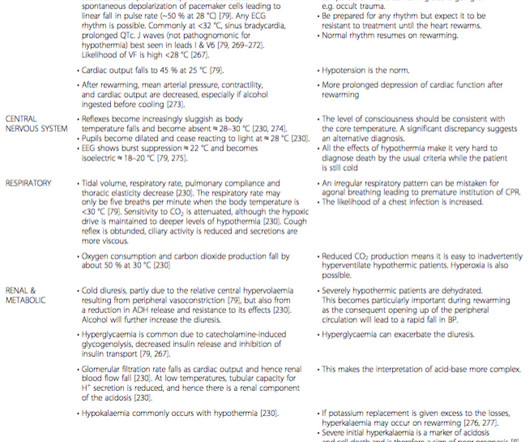
ERC 2015 guidelines recommend withholding adrenaline administration in hypothermic CA (HT IV) and limiting defibrillation to three attempts until the core temperature is >30 °C. ECLS has substantially improved survival and is the treatment of choice in the patient with unstable circulation or CA. Many arrhythmias (e.g.
The PEACH trial: No body had a fit, so… we have no clue Peter-Derex L, Philippeau F, Garnier P, et al. PMID: 30206143 Less is more when it comes to intravenous fluids de-Madaria E, Buxbaum JL, Maisonneuve P, et al. PMID: 35490863 Hands on defibrillation: Even if it’s safe, would it actually help? N Engl J Med.
Stredder et al, Archives of Disease in Childhood 2016 we see that 58% were not asked about triggers, 30% were not asked about duration and, importantly for risk stratification, 59% were not asked for a family history of cardiac disease. Palpitations (or descriptions thereof) are common but true arrhythmias are not.
She was given CRT-D (Cardiac Resynchronization Therapy-Defibrillator). For the majority of the tracing there are two P waves for each QRS. There is a LBBB. The PR interval gradually prolongs until a QRS is dropped and the pattern repeats itself. If there is no BBB the QRS will be narrow. There is for the most part 2:1 AV block.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She was immediately intubated during continued compressions, then underwent a 9th defibrillation, which resulted in an organized rhythm at 42 minutes after initial arrest. see below).
CPR is taken over by responding crews, and he is placed on a cardiac monitor/defibrillator. After several cycles of defibrillation, epinephrine, and amiodarone, the patient remains in cardiac arrest. Current AHA guidelines do not recommend routine use of calcium in cardiac arrest (Panchal, et al.,
Background: There are only two interventions that have been proven in the medical literature to improved outcomes in cardiac arrest: high-quality CPR and early defibrillation. Article: Moore JC et al. Over the years, we as a scientific community have worked extensively to find other interventions that improve outcomes.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content