This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. Lemkes JS, Janssens GN, van der Hoeven NW, et al.
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). The TOMAHAWK Investigators. first appeared on The Skeptics Guide to Emergency Medicine.
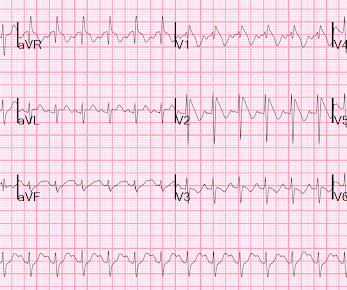
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby Emergency Department where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. He required multiple defibrillations within a period of a few hours. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. The below ECG was recorded. What do you think?
He underwent further standard resuscitation EXCEPT that we applied the Inspiratory Threshold Device ( ResQPod ) AND applied Dual Sequential Defibrillation (this simply means we applied 2 sets of pads, had 2 defib machines, and defibrillated with both with only a fraction of one second separating each defibrillation.
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
This ECG was read as “No STEMI” with no prior available for comparison. It is true this ECG does not meet STEMI criteria (there is 1.0 Armstrong et al. The Queen of Hearts sees it of course: Still none of these three ECGs meet STEMI criteria. Instead we discussed 5 minute delays for the STEMI(+) OMI patients.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. There is atrial fibrillation.
STEMI , ST-segment elevation acute myocardial infarction ). 1 Initial diagnosis of STEMI ECG Management Recommendation Level of evidence A 12-lead ECG should be interpreted immediately (within 10 minutes) at first medical contact. I B ECG monitoring should start immediately and a defibrillator must be ready.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She was immediately intubated during continued compressions, then underwent a 9th defibrillation, which resulted in an organized rhythm at 42 minutes after initial arrest. see below).
She was never seen to be in ventricular fibrillation and was never defibrillated. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Kurkciyan et al. BP gradually rose.
If it is STEMI, it would have to be RBBB with STEMI. Excerpted from Vutthikraivit et al: Acta Cardiol Sin 34:267-277, 2018 ). == Distinction is made between 2 types of Brugada ECG patterns: A B rugada - 1 ECG pattern — shows ≥2 mm coved ST elevation with sharp downslope plus T wave inversion in ≥2 anterior leads. Hypothermia.
She was defibrillated and resuscitated. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Lindahl et al. From Gue at al. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery.
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. In the largest study looking at this topic by Mizusawa et al., Bicarb 20, Lactate 4.2, Ammonia 100.
the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 How would you treat? I could find very little literature on the treatment of severe life-threatening hypokalemia. The estimated deficit associated with a serum decrease from 4.0
After epinephrine, atropine, and defibrillation x 2, there was a return of pulses. There is ST depression in II, III, and aVF that is concerning for reciprocal depression from high lateral STEMI in aVL, where there is some ST elevation. Plummer D et al. She collapsed and 911 was called; she was found pulseless.
Bayes de Luna, A et al. This is based on the Sieira et al, 2017, risk calculator , which gives a borderline risk score (2). An EP study might be helpful in symptomatic patients (Sroubek et al., Current electrocardiographic criteria for diagnosis of Brugada pattern: a consensus report. J Electrocardiology 45 (2012):433-442.
A 12-lead was recorded, showing "STEMI," but is unavailable. Moreover, if you know that catastrophic intracranial hemorrhage can result in an ECG that mimics STEMI, then you know that this patient probably has a severe intracranial hemorrhage. She was BVM ventilated and suctioned. Shortly thereafter, pulses were lost.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content