This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
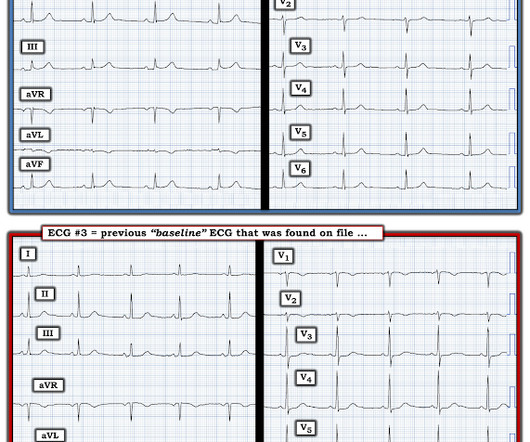
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. Deutch et al. Fortunately the patient did not reocclude while awaiting the angiogram.
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. de Winter et al in N Engl J Med 359:2071-2073, 2008. Cath attending is aware. Abstract 556.
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published.
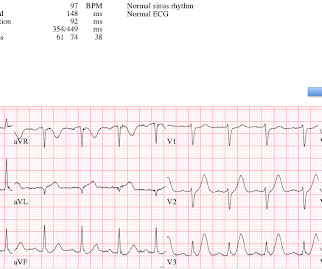
Figure 1-1 My colleague, a faithful student of ECG interpretation, handed me the tracing and said that it warranted STEMI activation because of apparent terminal QRS distortion (TQRSD) in V2. 1, 2] The most clinically useful definition to account for this entire constellation is intraventricular conduction delay.
They wanted to know if I would like them to activate the outside hospital's "STEMI alert." But of course, this is not a STEMI by definition as it does not meet STEMI criteria. They shot this ECG right before going into the ED: Clearly meets STEMI criteria with large STE in V2-V5. Here is the ECG: What do you think?
Lindahl et al. From Gue at al. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature.
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. Therefore, this does not meet the definition of myocardial infarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. You can see the deficiency of the definition of MI.
Here it is: Obvious Inferior Posterior STEMI (+) OMI. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.) The cath lab was activated prehospital But imagine if the patient had walked in.
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Although recognition of OMI was not affected by administration of morphine in this case, use caution with analgesia in ongoing ACS without a definitive plan for angiography. Bigger et al. Is there STEMI? Moffat, M.
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. They are definitely high in amplitude and, intermittently, appear to disproportionately tower over the respective QRS. Closer inspection will show that it is Sinus, after all. 2] Birnbaum, Y.,
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. She was out walking her dog when she developed sudden dizziness and light-headedness. When EMS found her, she was dyspneic and diaphoretic.
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Definition: total loss of R-wave means there is a QS-wave (a single deep deflection). He had a prehospital ECG: Obvious anterolateral acute STEMI The patient received aspirin only and his pain immediately resolved: Clear resolution of all ST elevation, with only some residual T-wave inversion in I and aVL. The LAD has reperfused early.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Herzog et al. Khan et al. Circulation 2007 2.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. There is no definite evidence of acute ischemia. (ie, In this study — Procainamide was superior to Amiodarone for terminating monomorphic VT, as well as having fewer adverse effects than Amiodarone ( Ortiz et al — Eur Heart J 1;38 (17): 1329-1335, 2017 ).
Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." And Olivier finishes with this commentary: "Yet another example in favor of abandoning STEMI criteria for diagnosing OMI. Peak troponin: 128,000 ng/L.
80%) and definitely too much for hour to hour. However, the Definition of MI requires at least one value above the 99th percentile, which for a male is 34 ng/L (16 ng/L for women). Heitner et al. Our patient already has an ECG diagnostic for OMI, so this finding is useless.) HsTnI drawn at that time was 9 ng/L (ref.
Validation of the Modified Sgarbossa Rule for Diagnosis of STEMI in the Presence of Left Bundle Branch Block. So there is a definite inferior and lateral MI. Meyers HP et al. Pendell is the lead author on our Modified Sgarbossa Criteria Validation Study. Limkakeng AT. Theiling BJ. 0 0 1 41 238 MMRF 1 1 278 14.0
Barely any STE, and thus not meeting STEMI criteria. Annals of Emergency Medicine Cardiology was called to evaluate the patient immediately for emergent cath, but they stated that the ECG did not meet STEMI criteria and elected to wait for further information before proceeding with cath. He was given 6mg IV morphine for ongoing pain.
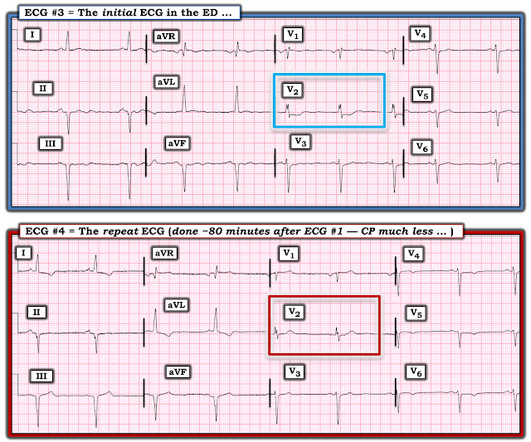
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
Troponin T peaked at 2074 ng/L (very high, typical of OMI/STEMI). Lead aVL is definitely not normal. Post PCI the patient became gravely hypotensive and "shocky". She stabilized on dobutamine and levosimendan infusions that could be discontinued after 24 hours. The LV EF was 57% at formal echo. 21, 2017 ).
Findings: - Sinus tachycardia - Poor R wave progression - STD in leads V3 and V4 - there is almost an appearance of STE in V6, but it is not definite - there is also slight STE in aVL with slight reciprocal STD in inferior leads Impression: Diagnostic of posterior OMI [and the subtle lateral involvement (aVL) supports this] until proven otherwise.
Based on recent studies, current guidelines recommend that O2 should not be given to non-hypoxemic patients with STEMI or NSTEMI [2,3]. Click here for Direct Download of the Podcast Paper: Stewart, RAH et al. 4159 patients (10% of total population) had STEMI 30d Mortality: High O2 protocol: 8.8% PMID: 25260718 Ibanez B et al.
Because there was proven thrombus (ACS) but the troponin never went above the 99% reference range (and therefore cannot be called MI -- definition of MI requires rise and/or fall of troponin with at least one value above the 99% reference range), this is UNSTABLE ANGINA with ST Elevation.
Article Summary by Sarah Fabiano, MD, FACEP, FAAEM Lyng JW, Braithwaite S, Abraham H, et al. Air medical transport has been utilized in multiple hospital based programs including trauma, STEMI, and stroke. Prehosp Emerg Care 2021 Nov-Dec;25(6):854-73. doi: 10.1080/10903127.2021.1967534.
Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Lindahl et al. From Gue at al. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery.
link] In this paper, in a department in which they state they have only 50 STEMI per year, they looked at only 8 days worth of triage ECGs for a total of 538. They did not find one STEMI on their triage ECGs (no surprise! We at HCMC have 30 walk-in STEMIs per year; the rest come by ambulance. Am J Emerg Med 36(10):1771-1774.
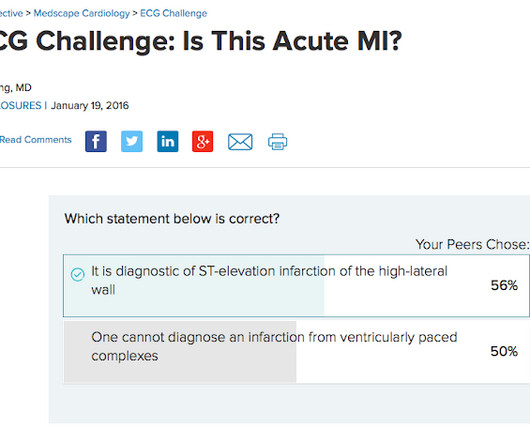
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI. Limkakeng AT.
Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Also note that they allow ST depression c/w posterior MI to be a STEMI equivalent. Kurkciyan et al. Kurkciyan et al.,
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). Hayakawa A, Tsukahara K, Miyagawa S, et al. In my opinion, I think it looks more like subendocardial ischemia. Am J Emerg Med.
Inferior ST Depression does NOT mean there is inferior subendocardial ischemia; it is generally reciprocal to high lateral (aVL) subepicardial ischemia (OMI/STEMI) == MY Comment by K EN G RAUER, MD ( 2/10/2023 ): == There are certain patterns in ECG interpretation that experienced providers are able to immediately recognize. See text ).
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Backus BE, Six AJ, Kelder JC, et al. Moumneh T, Sun BC, Baecker A, et al.
If it is STEMI, it would have to be RBBB with STEMI. Excerpted from Vutthikraivit et al: Acta Cardiol Sin 34:267-277, 2018 ). == Distinction is made between 2 types of Brugada ECG patterns: A B rugada - 1 ECG pattern — shows ≥2 mm coved ST elevation with sharp downslope plus T wave inversion in ≥2 anterior leads.
Khan AR, Golwala H, Tripathi A, et al. Acute myocardial infarction (AMI) was defined by the Third Universal Definition of AMI. And, in cases like the elderly patient with new-onset chest pain presented here — definitive diagnosis of acute STEMI is sometimes deceptively easy. In normal conduction , (i.e.,
The last section is a detailed discussion of the research on aVR in both STEMI and NonSTEMI. The additional ST Elevation in V1 is not usually seen with diffuse subendocardial ischemia, and suggests that something else, like STEMI from LAD occlusion, could be present. Here is an article I wrote: Updates on the ECG in ACS. see below).
Had the cardiologists followed NSTEMI or transient STEMI guidelines, which recommend non-urgent cath, the patient could have redeveloped an OMI and had a worse outcome. But this foresight will not be recorded, because the patient was diagnosed as "transient STEMI", even though no ECG ever met STEMI criteria.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. In the largest study looking at this topic by Mizusawa et al., So maybe she is better than I am. There was a 0.9% per year incidence of SCD in this cohort [1].
A recent study found that SCAD causes almost 20% of STEMI in young women. A study by Hassan et al. Lobo et al. examined SCAD presenting as STEMI (unlike Hassan et al. Lobo et al. examined SCAD presenting as STEMI (unlike Hassan et al. The SCAD cases in Lobo et al.
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? Physician interpretation: "No STEMI." Physician: "No STEMI." Cardiologist interpretation: "Technically does not meet STEMI criteria but concerning for ischemia."
4 Formerly, chest pain patients without an S-T Elevation Acute Myocardial Infarction (STEMI), whose pain was suspected to be cardiac in nature, became inpatients for sequential monitoring of their lactate dehydrogenase and creatine kinase isozyme profiles. Gulati M, et al. Stiell IG, et al. Stiell IG, et al. Postgrad Med.
This guideline revision is particularly timely as EMS systems have shown their abilities to dramatically improve survival and neurologic outcome after cardiac arrest, STEMI, acute stroke, and other time-sensitive conditions. References Lulla A, et al. Spaite DW, Bobrow BJ, Keim SM, et al. Prehosp Emerg Care. J Safety Res.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content