This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Chuck Pilcher, MD, FACEP Editor, Medical Malpractice Insights Editor, Med Mal Insights Excellent documentation supports standard of care, avoids lawsuit Vertebral artery CVA leaves patient disabled. Result : Based on excellent documentation of thoughtful medical decision making, the case was found to be defensible. UpToDate Online.
Reference: Knack et al. That document tells us “Before widespread implementation, CDRs should be compared to clinical judgement.” [3] A similar review by Sanders et al 2015 concludes that clinica. Early Physician Gestalt Versus Usual Screening Tools for the Prediction of Sepsis in Critically Ill Emergency Patients.
After 13 minutes of ALS resuscitation, pulses were palpated indicating a return of spontaneous circulation. The crew increases this current to 75mA and documents an “improvement in patient status” with palpated pulses and a BP of 115/60. Epinephrine administered intravenously. This set current is seen in Figure 5.
A critical MORSEL is that every child you treat for DKA needs to have an initial thorough neuro exam including cranial nerves and then frequent neuro reassessments … and document it ( so your colleagues who take over care for the kid can know if there has been a change )! PubMed] [Read by QxMD] Rosenbloom AL. 2013 Sep;163(3):761-6.
One of the first documented strikes among house staff officers took place in 1974 at Howard University here in Washington, D.C., Ahmed AM, Kadakia K, Ahmed A, et al. Historically, labor unionization among health care workers is uncommon, 5 including among resident physicians, 6 and the prospect of striking even more so. Beresford L.
Date: September 12, 2024 Reference: Anderson et al. These “allergies” are often poorly documented and could potentially be more accurately described as intolerance [1]. A pivotal study by Raja et al. Koo et al showed that offering amoxicillin oral challenges to ICU patients with low-risk penicillin allergies.
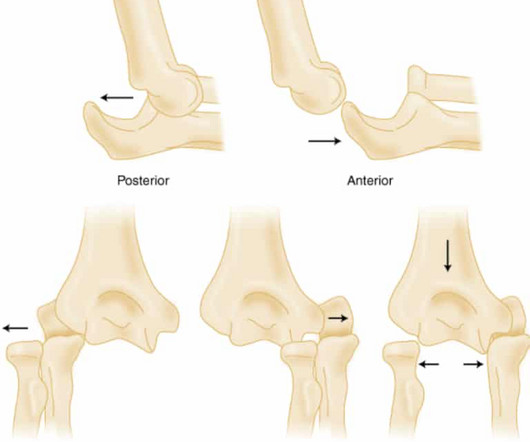
Commentary on an article by Marc Schnetzke, MD, et al.: “Determination of Elbow Laxity in a Sequential Soft-Tissue Injury Model. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. PMID: 28846302 O’Driscoll SW. How Do Elbows Dislocate?: A Cadaveric Study” J Bone Joint Surg Am. 17.01448.
Photographic documentation of the wound is helpful to enhance continuity of care. References Nussbaum SR, Carter MJ, Fife CE, et al. The ED case manager arranged follow up in the wound care clinic in two days. An economic evaluation of the impact, cost, and Medicare policy implications of chronic nonhealing wounds.
[display_podcast] Date: October 24th, 2017 Reference: Harrison et al. display_podcast] Date: October 24th, 2017 Reference: Harrison et al. That rant relied upon a Cochrane SRMA by Stevens B et al 2013 and a randomized clinical trail published in Pediatrics by Gray L et al 2015. Reference: Harrison et al.
13 Interventions may include: Ascertaining a patient’s preferred language early in the clinical encounter (during registration, for instance), and clearly documenting this preference in a place that is visible to all providers. Utilizing certified interpreters and documenting their use. Lion KC, et al. Regenstein M, et al.
Date: September 28th, 2022 Reference: Hartford et al. Date: September 28th, 2022 Reference: Hartford et al. Brown et al , Selbst and Clark ). It is not well documented, whether gaps in pain assessment and treatment exist in conditions in which opioids are not indicated, such as migraine headaches. AEM September 2022.
The nurse completes the Columbia-Suicide Severity Rating Scale (C-SSRS) and documents that the patient’s recent thoughts of killing himself and his detailed plan makes him “High Risk” for suicide. There is no documented handoff to the on-coming emergency physician (EP) who assumes care. Ronquillo L et al. Applebaum PS.
We collected data directly from the bedside clinician which enabled us to gather pertinent patient symptoms and physical examination findings that may not be well documented in the medical record, but more accurately identify the child’s injuries.” Baumann F, Ernstberger T, Neumann C, et al. Leonard JC, Harding M, Cook LJ, et al.
Reference: Pines et al. Reference: Pines et al. The American College of Emergency Physicians ( ACEP ) has a number of documents discussing APPs in the ED. Reference: Pines et al. Date: November 19th, 2020 Guest Skeptic: Dr. Corey Heitz is an emergency physician in Roanoke, Virginia. AEM November 2020. AEM November 2020.
Date: January 5th, 2021 Reference: Shipman et al. Date: January 5th, 2021 Reference: Shipman et al. The first documented use of topical ophthalmologic anesthetics was in 1818. We covered and randomized control trial by Waldman et al on topical tetracaine for simple corneal abrasions on SGEM#83.
A draft guidance document was developed after the completion of a national consultation process though an electronic survey with EMTs. Topics were selected by using section titles from the guidance document with a view to seeking further feedback and subsequent refinement of the proposals for CPD. MethodsWillis, et al.
The EMR tasks we undertake are expanding rapidly, far beyond simply documenting history and physical examination and every implementation slows us down. Research by Hill et al (1) demonstrated that an ED shift can have 4,000 clicks. Most emergency physicians use some form of electronic medical records (EMRs) when seeing patients.
Date: March 28, 2023 Reference: Fowler et al. Date: March 28, 2023 Reference: Fowler et al. You find her at the desk, asleep with her face on the keyboard, patient documentation half finished. Reference: Fowler et al. Objective assessment of sleep and fatigue risk in emergency medicine physicians.
An unknown EP reviews the report, determines that there is no reason to notify the patient, and documents nothing. It wasn’t, so you weren’t called, nor did the doc need to document anything. This patient’s history was either poorly taken or poorly documented. Baccei SJ et al. Tyler W et al. Volume 80, no.
Reference: Pines et al. The American College of Emergency Physicians ( ACEP ) also has a number of documents discussing APPs in the ED. Reference: Pines et al. Emergency Physician and Advanced Practice Provider Diagnostic Testing and Admission Decisions in Chest Pain and Abdominal Pain.
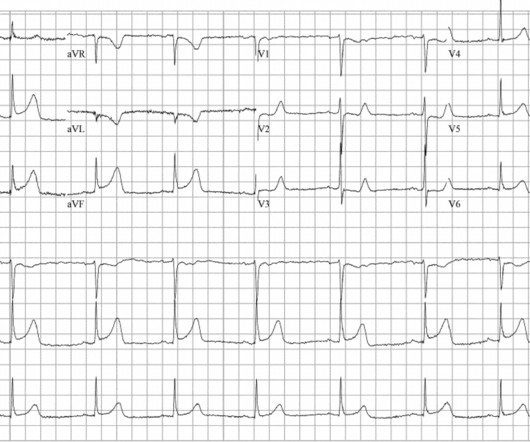
This case report documents the first known instance of using NTG during an emergency department resuscitation to treat a patient in cardiac arrest due to severe coronary artery vasospasm. Cardiac arrest secondary to myocardial ischemia from coronary vasospasm is well documented. References Prinzmetal M, Kennamer R, Merliss R, et al.
Date: May 6th, 2019 Reference: Sceats et al. Date: May 6th, 2019 Reference: Sceats et al. Case: An 18-year-old woman presents with a Grade 1 appendicitis (Tominaga et al J Trauma Acute Care Surg 2016). Background: The first documented appendectomy was done by Claudius Amyand in 1735. Reference: Sceats et al.
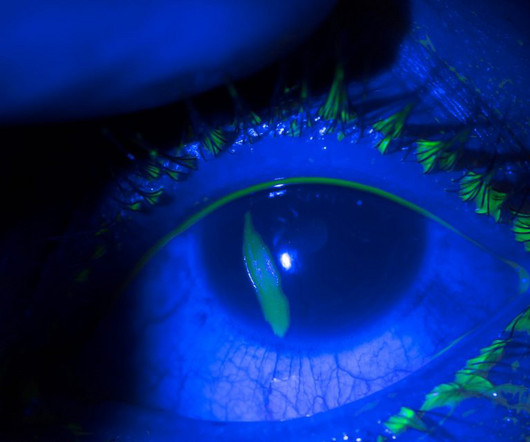
There is limited literature documenting eye involvement and pictographic examples of its presentation. The patient’s eye lesion and symptoms resolved and he was discharged on hospital day eight. Ocular lesions are a rare presentation of the monkeypox virus. The 2022 outbreak and the pathobiology of the monkeypox virus. J Autoimmun.
Brugada sign refers to the findings on ECG, while Brugada syndrome is the combination of ECG findings with one of the following: documented ventricular tachycardia or fibrillation, syncope, family history of sudden cardiac death at < 45 years old, or inducible ventricular tachycardia with programmed electrical stimulation. Circulation.
[display_podcast] Date: February 27th, 2018 Reference: Moran et al. display_podcast] Date: February 27th, 2018 Reference: Moran et al. Reference: Moran et al. Exclusions: There were 26 exclusions in their supplemental documentation. . Exclusions: There were 26 exclusions in their supplemental documentation.
Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. We documented that the majority of stenotic lesions had compensatory enlargement and thus exhibited remodeling.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. References: Jaff MR et al. PMID: 21422387 Wan S et al. PMID: 15262836 Sharifi M et al. PMID: 27422214 Wang C et al. PMID: 19741062 Kucher N et al. PMID: 24226805 Piazza G et al. PMID: 26315743 Tapson VF et al. CHEST 2010.
Document a risk and benefit discussion with the patient regarding empiric anticoagulation, perhaps even including the HAS-BLED score in the documentation [10]. References Kraaijpoel N, Carrier M, Le Gal G, et al. 0228788 Wells PS, Anderson DR, Rodger M, et al. Goldin Y, Pasvolsky O, Rogowski O, et al. Ultrasound.
[display_podcast] Date: September 10th, 2018 Reference: Gurley et al. display_podcast] Date: September 10th, 2018 Reference: Gurley et al. Reference: Gurley et al. Comparison of Emergency Medicine Malpractice Cases Involving Residents to Non-Resident Cases. first appeared on The Skeptics Guide to Emergency Medicine.
Date: November 30th, 2020 Reference: Ohle R et al. Date: November 30th, 2020 Reference: Ohle R et al. Over the past decade, some emergency physicians have adopted this examination into their own bedside clinical assessment and documentation. Reference: Ohle R et al. A Systematic Review and Meta-analysis.
Growdon ME, Jing B, Morris EJ, Deardorff WJ, Boscardin WJ, Byers AL, Boockvar KS, Steinman MA. Sponsor Freed is an AI scribe that listens, transcribes, and writes medical documentation for you. It turns clinicians’ patient conversations into accurate documentation – instantly. J Am Geriatr Soc. 2024 Jun;72(6):1728-1740.
Document the size, consistency and location in the notes to compare if they represent. References Al-Khateeb T, Al Zoubi F. 2006.11.039 Fanous A, Morcrette G, Fabre M et al. 2017.12.003 Machado De Carvalho G, Silva de Lavor M et al. They may grow again with subsequent upper respiratory tract infections.
Reference: Martel et al. Reference: Martel et al. Exclusions: Prisoners or those in police custody, pregnant or breast-feeding, or with documented allergy to any study medications. Exclusions: Prisoners or those in police custody, pregnant or breast-feeding, or with documented allergy to any study medications.
Date: April 24th, 2020 Reference: Watanabe et al. Date: April 24th, 2020 Reference: Watanabe et al. Reference: Watanabe et al. Is Use of Warning Lights and Sirens Associated With Increased Risk of Ambulance Crashes? A Contemporary Analysis Using National EMS Information System (NEMSIS) Data. Annals of Emergency Medicine.
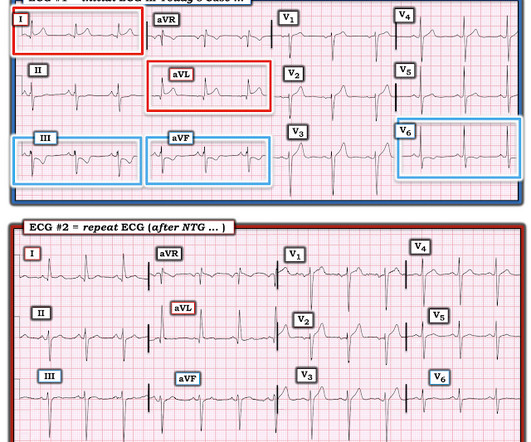
The documentation does not describe any additional details of the history. They also documented "Reproducible chest tenderness." Heitner et al. Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." The following ECG was obtained.
Kuttab et al’s findings, constituting 45% of the review’s weight, suggest that administering <30cc/kg IVF is associated with increased odds of mortality, delayed hypotension, and increased ICU utilization. Uchel et al’s contribution (21% weight) indicates that ≥30cc/kg IVF is linked to 2.5 2020;4(5):537-541.
The patient’s last INR should be documented, and one obtained if not recent. For patients on warfarin, documenting a reason for not checking an INR is a worthwhile practice. Baek BS et al. Vranckx P et al. This is a classic case of “anchoring bias” (i.e., References : 1. Spontaneous Spinal Epidural Hematoma.
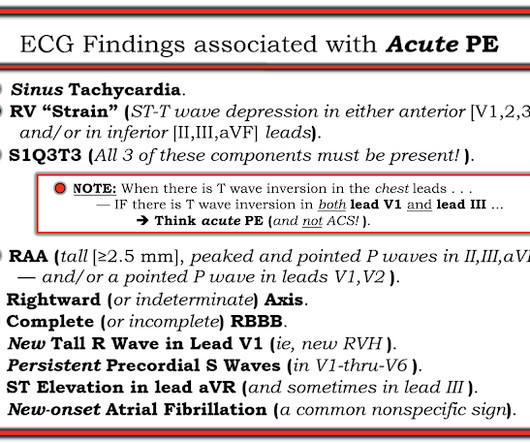
In fact, Kosuge et al. Stein et al. This is a paper worth reading : Marchik et al. Kosuge et al. Witting et al. This does not contradict the conclusions of Kosuge et al. found normal ECGs in only 3 of 50 patients with massive PE, and 9 of 40 with submassive PE. of patients with PE and 3.3% of controls.
Date: December 13th, 2021 Reference: Lee et al. Date: December 13th, 2021 Reference: Lee et al. Unfortunately, sexual harassment is also still widely documented in emergency medicine and has a major impact on career advancement and attrition [11-13].
Yes, temporize with supportive care while you go through the process, but do the work—find a legitimate representative or documentation of the patient’s wishes to determine what they’d want before you commit them to lengthy, aggressive life support. References Patel KK, Young L, Howell EH, et al. JAMA Intern Med.
Paper: Singer S, et al. References: Singer S, et al. PMID: 36108346 Cole JB, et al. PMID: 31270748 Maheshwari K, et al. PMID: 29872882 Jones AE, et al. PMID: 17035422 Holler JG, et al. PMID: 25789927 Schwartz MB, et al. The safety and efficacy of push dose vasopressors in critically ill adults.
This document is an update of guidelines first published in 2000, and then updated in 2007. Confounders to the GCS such as seizure and post-ictal phase, ingestions and drug overdose, as well as medications administered in the prehospital setting that impact GCS score should be documented. References Lulla A, et al. J Safety Res.
We’re defining “protocol” here as a written document that provides oversight from the medical director about how to assess and treat patients. Reassessment and Documentation After any type of restraint is instituted, careful assessment, re-assessment, and documentation is required. Was the documentation complete?
Pre-enrollment calculations estimated that 400 enrollments would be necessary to provide the trial with 80% power to detect a 15% difference in the primary outcome, allowing for up to 90 patients to be lost to follow-up or to have insufficient data documented. Reference: Ma H, Campbell BC, Parsons MW, et al. 2019; 380:1795-1803.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content