This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
After 13 minutes of ALS resuscitation, pulses were palpated indicating a return of spontaneous circulation. Crew notifies the received ED of an incoming post-arrest patient and notes a sinus bradycardia on their monitor, as seen in Figure 2. Pacing was continued in the ED, with identical settings. Several learning points here.
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. Chuck Pilcher, MD, FACEP Editor, Medical Malpractice Insights Editor, Med Mal Insights Excellent documentation supports standard of care, avoids lawsuit Vertebral artery CVA leaves patient disabled.
Reference: Knack et al. They were randomized to ceftriaxone 2gm intravenous (IV) in the ambulance or usual cares (fluids and supplementary oxygen) until arrive to the ED. That document tells us “Before widespread implementation, CDRs should be compared to clinical judgement.” [3]
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. Chuck Pilcher, MD, FACEP Editor, Medical Malpractice Insights Editor, Med Mal Insights The challenge of suicide evaluation in the ED “I’ve changed my mind. If you have a story to share click here.
About three percent of emergency department (ED) visits are due to skin and soft tissue infections, but data are lacking on the contribution of chronic wounds to this number. Wound management in the ED is only a starting point, and appropriate referral and follow-up are key to an improved outcome.
Date: September 12, 2024 Reference: Anderson et al. Case: It’s another day, another dollar in the emergency department (ED). You wonder if she could have an allergy challenge dose of ceftriaxone in the ED. These “allergies” are often poorly documented and could potentially be more accurately described as intolerance [1].
Date: September 28th, 2022 Reference: Hartford et al. Date: September 28th, 2022 Reference: Hartford et al. Patients with migraines often present to the ED looking for pain relief. Brown et al , Selbst and Clark ). Reference: Hartford et al. AEM September 2022. AEM September 2022. AEM September 2022.
Date: April 24th, 2020 Reference: Watanabe et al. This is Bob’s eleventh visit […] The post SGEM#291: Who’s Gonna Drive you to…the ED – with Lights & Sirens? This is Bob’s eleventh visit […] The post SGEM#291: Who’s Gonna Drive you to…the ED – with Lights & Sirens? Date: April 24th, 2020 Reference: Watanabe et al.
Reference: Pines et al. Reference: Pines et al. Case: You are the medical director of a medium sized urban emergency department (ED). The American College of Emergency Physicians ( ACEP ) has a number of documents discussing APPs in the ED. Reference: Pines et al. AEM November 2020. AEM November 2020.
6 24% more likely to return to the ED within 72 hours of their initial visit in an urban ED with >50,000 annual visits. 6 24% more likely to return to the ED within 72 hours of their initial visit in an urban ED with >50,000 annual visits. One cohort study in a public ED found that 84.5%
Reference: Pines et al. AEM January 2021 Case: A 50-year-old male presents to the Emergency Department (ED) with left lower quadrant abdominal pain. That SGEMHOP episode asked how the productivity of APPs compare to emergency physicians and what is its impact on ED operations? Reference: Pines et al.
Using this decision rule would have cut down on ED CT C-spine ordering by >50% in this derivation cohort. I am hopeful it will also improve the flow in the ED.” While plain films for C-spine injury had previously fallen out of routine ED practice, we now have more evidence to support their use in intermediate risk patients.
[display_podcast] Date: October 24th, 2017 Reference: Harrison et al. display_podcast] Date: October 24th, 2017 Reference: Harrison et al. That rant relied upon a Cochrane SRMA by Stevens B et al 2013 and a randomized clinical trail published in Pediatrics by Gray L et al 2015. Reference: Harrison et al.
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. Patient not informed of enlarged heart, dies 3 weeks post ED visit Miscommunicated radiology findings are a hot topic. Someone should have – either the first ED doc, the second ED doc, or my PCP.
The EMR tasks we undertake are expanding rapidly, far beyond simply documenting history and physical examination and every implementation slows us down. Research by Hill et al (1) demonstrated that an ED shift can have 4,000 clicks. SGEM#159 looked at the implementation of an EMR in a tertiary care ED.
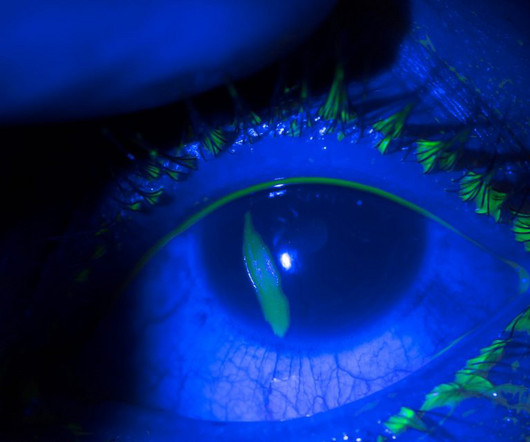
Date: January 5th, 2021 Reference: Shipman et al. Date: January 5th, 2021 Reference: Shipman et al. In the emergency department (ED), tetracaine drops are applied prior to slit lamp examination and the pain is completely resolved. The first documented use of topical ophthalmologic anesthetics was in 1818.
Takeaway lessons Many decisions in the ED are less about what to do, and more about when to do it. Takeaway lessons * Many decisions in the ED are less about what to do, and more about when to do it. Goals of care starts in the ED, and not with lip service. ICU time and ED time are different. JAMA Intern Med.
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. A CBC, Chem 7m and CT of the soft tissues of the neck are ordered by the departing ED doc whose clinical info for the radiologist is “facial swelling”. Baek BS et al. An INR is not done. References : 1.
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
Date: May 6th, 2019 Reference: Sceats et al. Date: May 6th, 2019 Reference: Sceats et al. Case: An 18-year-old woman presents with a Grade 1 appendicitis (Tominaga et al J Trauma Acute Care Surg 2016). Background: The first documented appendectomy was done by Claudius Amyand in 1735. Reference: Sceats et al.
This case report documents the first known instance of using NTG during an emergency department resuscitation to treat a patient in cardiac arrest due to severe coronary artery vasospasm. Cardiac arrest secondary to myocardial ischemia from coronary vasospasm is well documented. References Prinzmetal M, Kennamer R, Merliss R, et al.
Date: November 30th, 2020 Reference: Ohle R et al. Date: November 30th, 2020 Reference: Ohle R et al. Over the past decade, some emergency physicians have adopted this examination into their own bedside clinical assessment and documentation. Reference: Ohle R et al. A Systematic Review and Meta-analysis.
Johnson, MD ( Community EM, Salina Regional Health Center) // Reviewed by: Joshua Lowe, MD (EM Attending Physician, USAF); Marina Boushra, MD (Cleveland Clinic Foundation, EM-CCM); Brit Long, MD (@long_brit) Case A 40-year-old woman presents to a rural emergency department (ED) with left leg pain and swelling for the past 5 days.
Reference: Martel et al. Reference: Martel et al. AEM April 2021 * Population: Emergency department (ED) patients 18 years or old where the treating physician determined the need for parenteral sedation for acute agitation (it needed a patient or staff safety concern, not purely a high agitation score).
Date: December 13th, 2021 Reference: Lee et al. Date: December 13th, 2021 Reference: Lee et al. She has worked in five EDs so far, and a man has filled almost every leadership position. Addressing gender inequities: Creation of a multi-institutional consortium of women physicians in academic emergency medicine.
This time the team from Bristol Royal Children’s Hospital ED tell us what is new in the world of paediatric literature… Led by Dr John Coveney a Paediatric Emergency Medicine Trainee in Bristol who has revived The Journal Club at Bristol Royal Children’s Hospital ED on a monthly basis. Cochrane Database Syst Rev.
In fact, Kosuge et al. Stein et al. This is a paper worth reading : Marchik et al. Kosuge et al. Witting et al. This does not contradict the conclusions of Kosuge et al. found normal ECGs in only 3 of 50 patients with massive PE, and 9 of 40 with submassive PE. of patients with PE and 3.3% of controls.
A 36-year-old female presents to the ED after experiencing an episode of sudden syncope. Rosh Review Website Link References Antzelevitch C, Brugada P, Borggrefe M, et al. Priori SG, Napolitano C, Gasparini M, et al. Chen Q, Kirsch GE, Zhang D, et al. Wilde AA, Antzelevitch C, Borggrefe M, et al. Circulation.
Paper: Singer S, et al. This study chose a relevant topic to analyze that could influence acute management in the ED and has a fairly larger sample size of patients to do so. References: Singer S, et al. PMID: 36108346 Cole JB, et al. PMID: 31270748 Maheshwari K, et al. PMID: 29872882 Jones AE, et al.
Podcast: Play in new window | Download (Duration: 13:57 — 19.2MB) Subscribe: Apple Podcasts | Google Podcasts | RSS Management of the child with mental health problems who is boarding in the ED In episode 1 of this series, we discussed differentiating organic vs psychiatric causes of agitation in children.
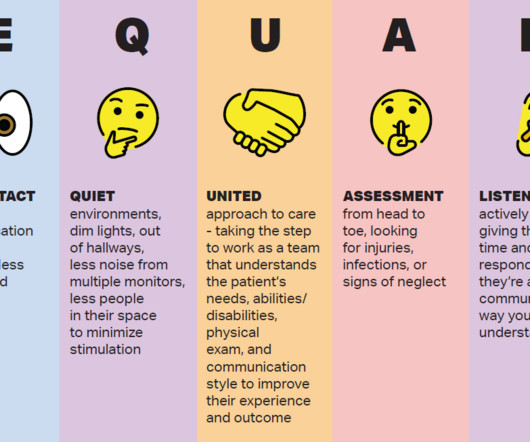
The care of patients with disabilities in the ED requires more attention, as not much data is available. Krahn, et al., highlight some discrepancies in experiences that may result in ED visits. 3 The need for this type of investigation was further highlighted in an article by York, et al. Krahn, et al.,
We’re defining “protocol” here as a written document that provides oversight from the medical director about how to assess and treat patients. Reassessment and Documentation After any type of restraint is instituted, careful assessment, re-assessment, and documentation is required. Was the documentation complete?
Prioritise listening to the first 30 minutes which given a good overview of aetiology and treatment (53 mins) Basics of cardiac rhythm problems in the ED Palpitations are a common reason for children to present to the emergency department, the majority of these will be benign from a cardiac perspective and instead related to stress or anxiety.
Well-designed multicentre large studies in children were warranted; cue Leonard et al. A proportion of the patients who were initially missed using the CDR were found to actually have risk factors documented in EMS reports or the medical record. I am hopeful it will also improve the flow in the ED.”
Malhotra et al. Regan et al. You receive a referral for a 7-year-old Josh, who presented to the emergency department (ED) with a 5-day history of fever, cough, and borderline oxygen saturation. The ED clinician made an impression of a chest infection. Lina Jankauskaite, Grechukha Y, Kjær KA, et al. BMJ Qual Saf.
A medical student reports a murmur, not documented by either the emergency physician or the cardiologist. In the ED, his troponin, ECG, and chest X-ray (CXR) are normal. An aortic dissection is discovered when he bounces back to the ED. He arrives in the ED stating, “I can’t move my legs.” References Hansen MS, et al.
Paper: Lema GMC, De Leacy R, Fara MG, et al. The protocol involved collaboration between the ophthalmology service, ED, and stroke service, including neurology and neuroendovascular teams. Outside eye care providers could refer patients directly to the ED for expedited evaluation. PMID: 32568646 Wang X, Liu Y, Suo Y, et al.
Background: Atrial fibrillation and atrial flutter with rapid ventricular rate (AF/AFL with RVR) are the most common subtypes of SVT, comprising a large number of ED visits in aging populations. Article: Rossi N et al. The study was dependent on EMR documentation which is prone to error. Am J Emerg Med.
The Queen of Hearts agrees: Here the Queen explains why: However, it was not interpreted correctly by the providers: ED interpretation of ECG: "paced rhythm, LBBB but no STEMI pattern." Available from: [link] If you are wondering about the Barcelona rule, then you should read the above paper by Khawaja et al. 2021;23:187.
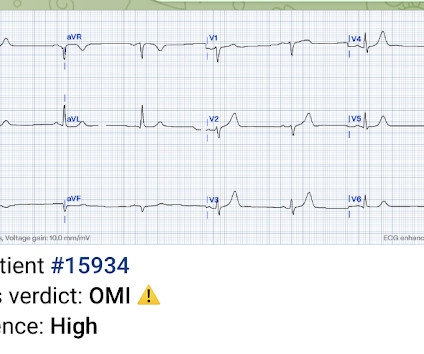
Dr. Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al. Patient 1 : anterior OMI Compared with baseline (first ECG), the initial ED ECG (second ECG) has mild ST elevation and hyperacute T waves V2-3 and mild ST depression in V6.
Over the past few years, there has been an increase in emergency department (ED) volumes and lengths of stay. The result of this ED capacity strain and less than ideal patient to staff ratios has led to delays in interventions, treatments and care adjustments. Paper: Owyang CG, et al. J Crit Care.
Algorithm: Marquette 12 SL (GE) The Queen gets it right Case 9 (prehospital and ED ECGs). The Queen gets it right First ED ECG: Hyperacute T-waves persist. Echocardiography, even (or especially) with Speckle Tracking, can get you in trouble. The ECG told the story. 30 yo woman with trapezius pain. HEART Pathway = 0.
3 Case 1: Posterior Stroke Presenting as Food Poisoning A 42-year-old man presents to the emergency department (ED) with sudden onset of severe vertigo, headache, nausea, and vomiting after eating Italian food. On arrival in the ED, symptoms have resolved except for the headache. References Kattah JC, Talkad AV, Wang DZ, et al.
Article 1: Positive urine cultures without pyuria Wang ME, Jones VG, Kane M, et al. of patients with follow-up documentation, 70.8% (95% CI 62.9–77.9) Reviewed by: Sarah Gentle and Owen Hibberd Article 2: Second attempt success in neonatal intubation Johnson MD, Tingay DG, Perkins EJ et al. Arch Dis Child Fetal Neonatal Ed.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content