This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published.
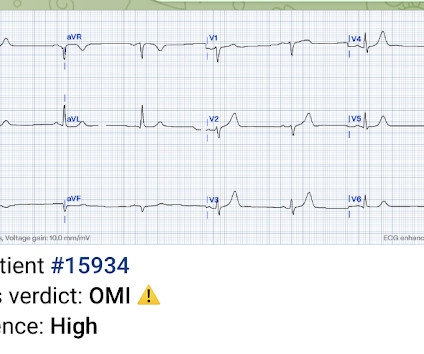
Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al. This is diagnostic of LAD occlusion but is equivocal for STEMI criteria and was missed (and both labeled ‘normal’ by final cardiology interpretation).
Unknown algorithm The Queen gets it right Case 4 How unreliable are computer algorithms in the Diagnosis of STEMI? The patient's prehospital ECG showed that there was massive STEMI and these are hyperacute T-waves "on the way down" as they normalize. Pain was resolving. Diagnosed as Normal by the computer. Troponin negative.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. He was started on nitro gtt.
The Queen of Hearts agrees: Here the Queen explains why: However, it was not interpreted correctly by the providers: ED interpretation of ECG: "paced rhythm, LBBB but no STEMI pattern." Most large STEMI have peak troponin I in the 20.0 Next trop in AM. Peak trop 257.97 Smith: This is an enormous myocardial infarction. ng/mL - 80.0
He had no previously documented medical problems except polysubstance use. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Bigger et al. Is there STEMI? Sadowski ZP, Alexander JH, Skrabucha B, et al. The patient continued having chest pain. Leave it alone.
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." In fact, Kosuge et al. Stein et al. This is a paper worth reading : Marchik et al. Kosuge et al. Witting et al. of patients with PE and 3.3% of patients without PE.
The documentation does not describe any additional details of the history. They also documented "Reproducible chest tenderness." Heitner et al. Written by Willy Frick A 46 year old man with a history of type 2 diabetes mellitus presented to urgent care with complaint of "chest burning." The following ECG was obtained.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. In both tracings — an exceedingly fast PMVT is documented. In this study — Procainamide was superior to Amiodarone for terminating monomorphic VT, as well as having fewer adverse effects than Amiodarone ( Ortiz et al — Eur Heart J 1;38 (17): 1329-1335, 2017 ).
This document is an update of guidelines first published in 2000, and then updated in 2007. Confounders to the GCS such as seizure and post-ictal phase, ingestions and drug overdose, as well as medications administered in the prehospital setting that impact GCS score should be documented. References Lulla A, et al.
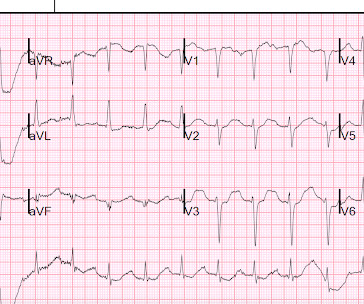
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 It is well documented with continuous 12-lead monitoring that acute re-occlusion is frequently asymptomatic.
STEMI , ST-segment elevation acute myocardial infarction ). 1 Initial diagnosis of STEMI ECG Management Recommendation Level of evidence A 12-lead ECG should be interpreted immediately (within 10 minutes) at first medical contact. I C If possible, patients should bypass non-PCI centres to a PCI-capable centre.
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
Based on recent studies, current guidelines recommend that O2 should not be given to non-hypoxemic patients with STEMI or NSTEMI [2,3]. Click here for Direct Download of the Podcast Paper: Stewart, RAH et al. 4159 patients (10% of total population) had STEMI 30d Mortality: High O2 protocol: 8.8% PMID: 25260718 Ibanez B et al.
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." Physician interpretation: "No STEMI."
Article Summary by Sarah Fabiano, MD, FACEP, FAAEM Lyng JW, Braithwaite S, Abraham H, et al. Appropriate air medical services utilization and recommendations for integration of air medical services resources into the EMS system of care: a joint position statement and resource document of NAEMSP, ACEP, and AMPA.
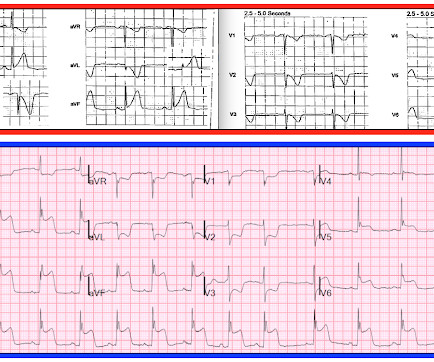
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. Our patient had a Brugada Type 1 pattern elicited by an elevated core temperature, which is also a documented phenomenon. So maybe she is better than I am. There was a 0.9%
4 Formerly, chest pain patients without an S-T Elevation Acute Myocardial Infarction (STEMI), whose pain was suspected to be cardiac in nature, became inpatients for sequential monitoring of their lactate dehydrogenase and creatine kinase isozyme profiles. Gulati M, et al. Stiell IG, et al. Stiell IG, et al. Postgrad Med.
He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." See far below for data on 24 troponin T in STEMI and NSTEMI, and correlation with infarct size. This difficulty results in high lateral OMI being the most commonly missed OMIs by the misguided STEMI criteria. From AM et al.
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. Comment by KEN GRAUER, MD ( 7/11/2018 ): = Insightful blog post by Dr. Smith regarding ECG criteria for recognizing acute RV involvement in patients with inferior STEMI. But which myocardial walls are affected?
Discussion See this post: STEMI with Life-Threatening Hypokalemia and Incessant Torsades de Pointes I could find very little literature on the treatment of severe life-threatening hypokalemia. Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia." mEq/L to 3.0 mEq/L to 2.0
Authors state early cath may be of benefit in those with no STEMI, but much of the more recent literature suggests this is more controversial. These conversations should occur frequently and be clearly documented for other health care professionals who are not present during the conversations (96%, 22/23).
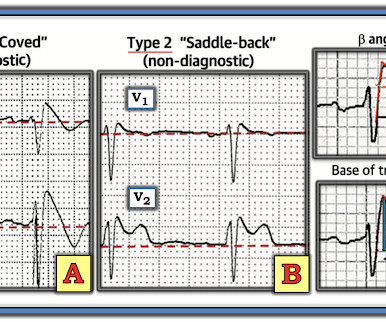
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. In the largest study looking at this topic by Mizusawa et al., Bicarb 20, Lactate 4.2, Ammonia 100.
Document in the patient's chart that rapid infusion is intentional in response to life-threatening hypokalemia." the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 If cardiac arrest from hypokalemia is imminent (i.e.,
STEMI negative : the EMS automated interpretation read, “STEMI negative. According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. Inferior infarct, age undetermined.
Thus, Brugada is the likely diagnosis _ A very nice explanation of this is given in the document quoted below on current ECG criteria for Brugada pattern. Bayes de Luna, A et al. This is based on the Sieira et al, 2017, risk calculator , which gives a borderline risk score (2). J Electrocardiology 45 (2012):433-442.
There is very scarce documentation, but the next ECG was obtained around 1 PM. Limitations of registry data: This patient presented with STEMI (-) OMI and developed STEMI the following day. In the world of STEMI, we are incapable of recognizing the first ECG as a false negative. A recent meta-analysis by Stone et al.
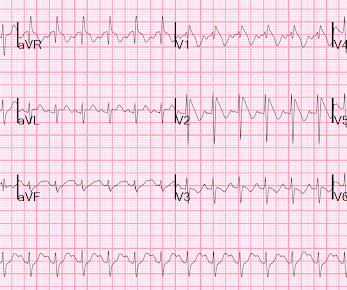
Unexplained cardiac arrest or documented VF/polymorphic VT: +3 3. How well does the computer interpretation perform? -- in this case, the computer diagnosed STEMI but the patient had Fever with Brugada -- A young F is hyperthermic, delirious, and dry: Fever-induced Brugada? Clinical History 2.a. syncope of unclear etiology: +1 2.c.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content