This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Your medical team is great, but you […] The post SGEM#250: Scribes – I Want to Break Free (from the EMR) first appeared on The Skeptics Guide to Emergency Medicine. Most emergency physicians use some form of electronic medical records (EMRs) when seeing patients. SGEM#159 looked at the implementation of an EMR in a tertiary care ED.
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP).
Date: June 2nd, 2020 Reference: Permpikul et al. Date: June 2nd, 2020 Reference: Permpikul et al. Case: It’s another day in your emergency department (ED). The triage nurse places a 61 year-old-man with fever, hypotension, cough into the smallest room in the ED. Reference: Permpikul et al.
By Smith, peer-reviewed by Interventional Cardiologist Emre Aslanger Submitted by anonymous A 53 y.o. male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. The pain radiated to both shoulders.
Background: Atrial fibrillation and atrial flutter with rapid ventricular rate (AF/AFL with RVR) are the most common subtypes of SVT, comprising a large number of ED visits in aging populations. Article: Rossi N et al. The study was dependent on EMR documentation which is prone to error. Am J Emerg Med.
5 Paper: Lebin J et al. Electronic Health Record (EHR) database review using keywords for demographics, triage vital signs, and administered medications. History of liver disease, history of substance abuse disorder, and history of delirium tremens were also extracted from the hospital EMR. J Med Toxicol 2022.
Paper: Singer S, et al. This study chose a relevant topic to analyze that could influence acute management in the ED and has a fairly larger sample size of patients to do so. References: Singer S, et al. PMID: 36108346 Cole JB, et al. PMID: 31270748 Maheshwari K, et al. PMID: 29872882 Jones AE, et al.
Over the past few years, there has been an increase in emergency department (ED) volumes and lengths of stay. The result of this ED capacity strain and less than ideal patient to staff ratios has led to delays in interventions, treatments and care adjustments. Paper: Owyang CG, et al. J Crit Care.
This was contributed by Co-editor Emre Aslanger, an interventional cardiologist in Turkey. This 65-year old male patient with severe underlying coronary disease presented to the ED after receiving several ICD shocks.
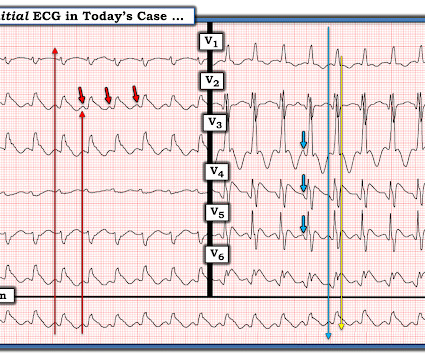
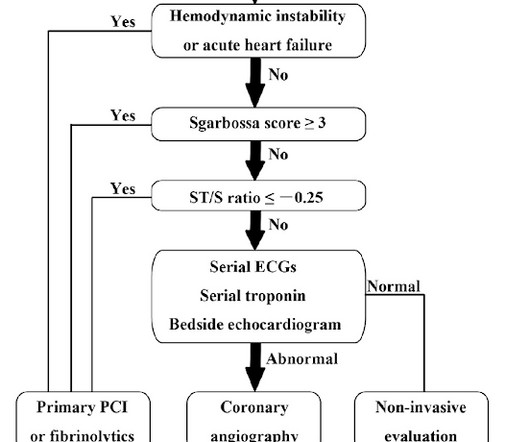
The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Below is the first ED ECG, labeled LBBB by the machine. In this case, cardiology noted “old LBBB, negative Sgarbossa”, so they kept the patient in the ED for repeat ECGs and troponin levels. Vitals were HR 58 BP 167/70 R20 sat 96%.
Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Lindahl et al. From Gue at al. Lindahl B, Baron T, Erlinge D, et al. To Emphasize: The reason definitive diagnosis is important in today's case — is that the senior ED physician interpreted ECG #1 as "nothing too exciting". References: 1.
To assess the clinical impact and relevance of these concerns, Alwang et al. Reliance on a billing dataset, instead of EMR or prospective data, likely affected the quality of outcome measurement. PMID: 28423290 Kidwell K, Albo C, Pope M, et al. Characteristics of sickle cell patients with frequent ED visits and hospitalizations.
While this guide isnt exhaustive, its designed by residents, for residents, to provide practical tips and foundational knowledge thats crucial in the fast-paced, high-stakes environment of the ED. Introduction Airway management is a critical ED skill to master. History When did they last eat (aspiration risk)?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content