This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Epinephrine administered intravenously. After 13 minutes of ALS resuscitation, pulses were palpated indicating a return of spontaneous circulation. They administered 10 mcg of push-dose epinephrine. Atropine and further doses of epinephrine were not administered. Pacing was continued in the ED, with identical settings.
Epinephrine and cardiac arrest: what’s the question? How much epinephrine is enough? Garcia et al. published a retrospective study in AJEM discussing cumulative epinephrine dosage in cardiac arrest.
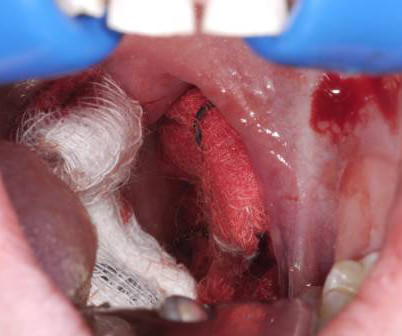
A young woman, 13 days post-tonsillectomy, comes into your rural emergency department (ED) coughing up blood. Managing post-tonsillectomy hemorrhage in the ED can be challenging, especially in rural or resource-limited settings. References Grasl S, Mekhail P, Janik S, et al. Dharmawardana N, Chandran D, Elias A, et al.
Date: September 18, 2024 Reference: Dillon et al. He currently practices emergency medicine in New Mexico in the ED, in the field with EMS and with the UNM Lifeguard Air Emergency Services. You and your partner initiate high-quality CPR, place a supraglottic airway, establish intra-osseous (IO) access and administer epinephrine.
Both norepinephrine and epinephrine can be used. Epinephrine is key if there is significant bradycardia. Tenenbein M, Macias CG, Sharieff GQ, et al, eds. Tenenbein M, Macias CG, Sharieff GQ, et al, eds. Crystalloid may help, but neurogenic shock may not respond to fluid administration. 5 th Edition.
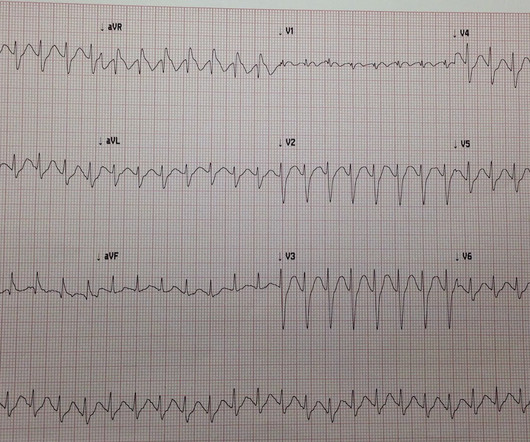
After administering 1mg of epinephrine ROSC is noted with a bradycardic rhythm ( Figure 2 ). On ED arrival ROSC is achieved. The University of Maryland found that capture occurred in only 42-78% of patients, dependent on pad positioning (Moayedi et al, 2022). Junctional Rhythm, occasional PAC's, and artifact.
How Long Should We Monitor After Giving IM Epinephrine for Anaphylaxis? Bottom Line Up Top: After prompt recognition and appropriate treatment with IM epinephrine, the risk of biphasic reactions are exceedingly low. At the time of discharge, appropriate patient education and prescriptions for IM epinephrine are essential.
1-4 The PDPs, phenylephrine and epinephrine, result in vasoconstriction and increased cardiac contractility. They can be associated with side effects such as reflex bradycardia, decreased stroke volume in phenylephrine, tachycardia and hypertension associated with epinephrine. Paper: Singer S, et al. Am J Emerg Med. 2022 Sep 5.
Sinha 2012] It is useful in the prehospital setting , correlating well with actual weight and ED Broselow weight. Most emergency drugs except for amiodarone and succinylcholine are based on ideal body weight [Emergency Medical Services for Children, Luten 2007] Epinephrine, dopamine, fentanyl, ketamine based on what child should weigh.
Date: November 10th, 2021 Reference: Andersen, et al: Effect of Vasopressin and Methylprednisolone vs Placebo on Return of Spontaneous Circulation in Patients With In-Hospital Cardiac Arrest. Case: A code blue is called for a 71-year-old male in-patient that is boarding in the emergency department (ED). JAMA Sept 2021. JAMA Sept 2021.
1 2 3 4 This article will focus on three lower extremity (LE) nerve blocks commonly used for acute lower extremity pain in the ED. link] [3] Morrison RS, Magaziner J, Gilbert M, et al. Door-to-block time: prioritizing acute pain management for femoral fractures in the ED. J Gerontol A Biol Sci Med Sci. 2003;58(1):76-81.
Xylazine is an alpha-2 agonist similar to clonidine that inhibits the release of norepinephrine and epinephrine resulting in decreased vascular tone and heart rate [4]. PMID: 34529640 Ayub S, Parnia S, Poddar K, et al. PMID: 24769343 Ehrman-Dupre R, Kaigh C, Salzman M et al. PMID: 36148197 Love JS, Levine M, Aldy K, et al.
Date: January 5th, 2021 Reference: Grunau et al. Date: January 5th, 2021 Reference: Grunau et al. Case: During a busy emergency department (ED) shift the paramedic phone rings. Reference: Grunau et al. first appeared on The Skeptics Guide to Emergency Medicine.
Reference: Cashen K, Reeder RW, Ahmed T, et al. Reference: Cashen K, Reeder RW, Ahmed T, et al. Case: A 6-month-old boy presents to the emergency department (ED) with three days of worsening cough, cold symptoms, and fever. Background: We often manage patients in cardiac arrest in the ED or the intensive care unit (ICU).
emergency departments (EDs), with statistics reporting more than 356,000 out-of-hospital cardiac arrests per year. 2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. References Tsao CW, et al. Benjamin EJ, et al. Kimblad H, et al.
The book Buy the new textbook (Bryan edited, Brandon authored a chapter) here or on Amazon: Concepts in Surgical Critical Care, First Edition ed. To hemodynamically manage RV failure without worsening RV afterload, consider the Rule of 8s cocktail:* Epinephrine.08 Figure 1 from Srour et al (vide infra).
Read More EMCrit: Podcast 145 – Awake Intubation Lecture from SMACC ERCast: Angioedema References: Baş M et al. PMID 25629740 Hassen GW et al. PMID 23062323 Kostis JB et al. PMID 16043683 McCormick M et al. PMID 20954277 Sinnert R et al. Zuraw et al. In: UptoDate, Feldweg AM (ed.) N Engl J Med.
These medications are a vital tool in the care of ED patients, from simple local analgesia for a laceration repair to regional analgesia for painful procedures. 1,2] Consider using a physiological marker to help identify inadvertent vascular injection, such as epinephrine. [3] doi:10.1007/BF03161199 Olson K, Smollin C, eds.
Louis) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) Case You are working in the trauma/critical care pod of your emergency department (ED). His blood sugar was normal en route to the ED, and his initial rhythm on the cardiac monitor was asystole. Carsten L, et al. Forti A, Brugnaro P, Rauch S, et al.
Traditional Advanced Cardiovascular Life Support (ACLS) medications, namely epinephrine, have been known to exacerbate coronary vasospasm. Dr. Rad is ED faculty at Wellstar Kennestone Regional Medical Center in Marietta, Ga., References Prinzmetal M, Kennamer R, Merliss R, et al. Myerburg RJ, Kessler KM, Mallon SM et al.
A gravid woman presents to your emergency department (ED). mg/kg IV epinephrine, or 0.05–0.1 Aziz K, Lee HC, Escobedo MB, et al. Before you can obtain any history, she gives birth in your waiting room. The neonate is apneic and has a heart rate of 48. How do you stabilize this patient? ET tube size should be 2.5 2016;8:11-19.
Article: Abella BS et al. Key Secondary Endpoints: 5 (3.9%) patients in the IV cetirizine group returned to any ED or clinic within 24 hours compared to 15 (11.1%) in the IV diphenhydramine group; P=0.04 Anecdotally, the persistence of urticaria often has little influence on the decision to discharge a patient from the ED.
When simple maneuvers fail, we proceed to topical agents such as lidocaine with epinephrine, oxymetazoline, anterior nasal packing, and electrical or chemical cauterization. TXA has become the standard practice in the ED based on small RCTs, though larger trials have not demonstrated the same benefit ( REBEL EM review ).
When simple maneuvers fail, we proceed to topical agents such as lidocaine with epinephrine, oxymetazoline, anterior nasal packing, and electrical or chemical cauterization. TXA has become the standard practice in the ED based on small RCTs, though larger trials have not demonstrated the same benefit (REBEL EM review). Am J Emerg Med.
One of the most hair-raising presentations to the emergency department (ED) can be massive hemoptysis with respiratory failure. Atchinson PRA, Hatton CJ, Roginski MA, et al. Ittrich H, Bockhorn M, Klose H, et al. Li H, Ding X, Zhai S, et al. Kathuria H, Hollingsworth HM, Vilvendhan R, et al. 2021;42(1):145-159.
The data in the paper by Rangel et al. Lange RA, Cigarroa RG, Flores ED, et al. McCord J, Jneid H, Hollander JE, et al. Esmolol in the management of epinephrine- and cocaine-induced cardiovascular toxicity. is intuitive, and not surprising. Vittinghoff, E. ADDIN EN.CITE Lange 1990 734 734 17 Lange, R.A. McBride, W.
Casey The CLOVERS trial: National Heart, Lung, and Blood Institute Prevention and Early Treatment of Acute Lung Injury Clinical Trials Network; Shapiro NI, Douglas IS, Brower RG, et al. Epinephrine metered-dose inhaler for pediatric croup. Early Restrictive or Liberal Fluid Management for Sepsis-Induced Hypotension. N Engl J Med.
With ventilations and epinephrine, she regained a pulse. She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR. Kurkciyan et al.
Fine ventricular fibrillation She received 2 mg epinephrine, 150 mg amiodarone and underwent chest compressions with the LUCAS device. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. see below). I have never seen this, but it is possible.
This is a 30-something healthy patient presented with COVID pneumonia who presented to the ED. He underwent CPR, and regained a pulse after epinephrine, with an organized narrow complex rhythm at 140, but still with severe shock. 3–8 Shi et al. Sandoval Y, Smith SW, Sexter A, et al. Shi S, Qin M, Shen B, et al.
The patient was brought directly to the cardiac catheterization lab for PCI, bypassing the ED. Dobutamine may be preferred in patients without severe hypotension who have high vascular resistance. -- De Backer D et al. Taglieri N, Marzocchi A, Saia F, et al. Kosuge M, Ebina T, Hibi K, et al. Richard, C; et al.
Here is his ED ECG: There is obvious infero-posterior STEMI. the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. Hypokalemia after cardiac arrest was independent of arterial pH, epinephrine or bicarbonate therapy during resuscitation, or prior therapy with diuretic drugs, digoxin or propranolol.
On arrival to the ED, her blood pressure is 84/36 mmHg with a heart rate of 110 beats per minute. 3,4 Prompt recognition and management of sepsis and septic shock are paramount for the ED clinician. 8,9 Recently, monocyte distribution width (MDW) has shown promise in a large meta-analysis as a useful screening tool in the ED.
Other Norepinephrine or epinephrine are preferred vasopressors when needed. In: Brent J, et al. Eds (2017). Starr P, Klein-Schwartz W, et al. e4 Livshits Z, Feng Q, Chowdhury F, et al. Gosselin S, Hoegberg L, Hoffmann R, et al. PMID: 26856351 Stranges D, Lucerna A, Espinosa J, et al. Wu P, Juurlink D.
Dell KM, et al. Eisen S et al. Fielder AR, et al. Arch Dis Child Fetal Neonatal Ed. Arch Dis Child Fetal Neonatal Ed. Bm MV, et al. Toepfner N, et al. Toniutti M, et al. Meoli M, et al. Ashton JJ, et al. Ding G et al. Tanti DC, et al. Ahlqvist VH, et al.
A 67-year-old man presents to the emergency department (ED) in cardiac arrest. Multiple attempts at defibrillation, epinephrine, and amiodarone have been unsuccessful. On ED presentation, he is unresponsive and the monitor shows ventricular fibrillation. References Go AS, Mozaffarian D, Roger VL, et al. Circulation.
Sex ed” sucks. They believe that Sex Ed programs are irrelevant to real-life experience and contain inadequate discussion of important issues, including consent or positive sexual relationships. Nizami T, Beaudoin F, Suner S, et al. Disease relapse should not automatically be assumed to mean failure of therapy. Crocker, B.C.S.,
Prior to this intervention, management in the ED is mainly supportive of the patient’s hemodynamic and cardiac status. Rosh Review Website Link Further Reading Further FOAMed: [link] [link] References: Ahmad SA, Brito D, Khalid N, et al. doi:[link] Kosuge M, Ebina T, Hibi K, et al. Takotsubo Cardiomyopathy. 2014;8:CMC.S14086.
A 43-year-old male with a history of mitral valve regurgitation s/p valvular replacement, hypertension, hyperlipidemia was evaluated in the ED for septic shock secondary to a pyelonephritis with a renal abscess. doi:10.1016/S0033-0620(05)80036-2 Balik M, Novotny A, Suk D, et al. doi:10.1136/BCR-2018-225879 Dawood S, Hill A, Al Rawi O.
This is what the providers in the ED understood on patient arrival: Patient called 911 for syncope, then had witnessed PEA arrest after medics arrived. Resuscitated with chest compressions, epinephrine. including epinephrine, and there was ROSC. Not a shockable rhythm. Resuscitation was begun with chest compressions, etc.,
In the ED, he develops recurrent respiratory depression and hypoxia to 80%. How long should they stay in the ED? DOI: [link] O’Donnell J, Tanz LJ, Miller KD, et al. Al-Azzawi M, Alshami A, Douedi S, Al-Taei M, Alsaoudi G, Costanzo E. Available at: [link] October 19, 2023 Kelly A, Kerr D, Dietze P, et al.
Airway: Key decision: base decision for intubation on clinical course, efficacy of airway clearance (coughing, mental status), ED/institutional resources, respiratory status (respiratory failure). Bronchoscopy can be used for bleeding control with cold saline, epinephrine, activated factor VIIa, or TXA. Am J Emerg Med. Am J Emerg Med.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content