This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Hosts: Joe Offenbacher, MD Audrey Bree Tse, MD [link] Download Leave a Comment Tags: Anticoagulation , Critical Care , Resuscitation Show Notes Coagulation Cascade: Algorithm for Anticoagulated Bleeding Patient in the ED: Indications for Anticoagulation Reversal: References: Baugh CW, Levine M, Cornutt D, et al. Ann Emerg Med.
It’s a busy day in the paediatric ED. The osmolar gap measures the difference between the measured plasma osmolality and the calculated plasma osmolality , providing an estimate of unmeasured solutes in the blood. Glucose] is the plasma glucose concentration (mg/dL). Back to our toddler in the ED. N Engl J Med.
Date: June 12th, 2022 Reference: Finfer et al. Date: June 12th, 2022 Reference: Finfer et al. sodium chloride), and balanced crystalloid solutions, meaning those with a chloride composition closer to plasma such as lactated ringer’s or Plasma Lyte 148. Reference: Finfer et al.
Date: June 18th, 2022 Reference: Crombie et al. Date: June 18th, 2022 Reference: Crombie et al. He is also now a fully fledged “sonologist” Casey currently splits his time between Broome, a small rural hospital in the remote Kimberley region of Western Australia, and a large tertiary ED in sunny Perth.
mental status, urine output, capillary refill) is more important than an actual goal PERMISSIVE HYPOTENSTION IN PTS WITH TBI Brotfain E et al. mental status, urine output, capillary refill) is more important than an actual goal PERMISSIVE HYPOTENSTION IN PTS WITH TBI Brotfain E et al. Richards JE et al. NEJM 1994. [2]
Date: December 16th, 2022 Reference: Hohle et al. Date: December 16th, 2022 Reference: Hohle et al. Case: A 71-year-old man is brought to your emergency department (ED) by emergency medical serviced (EMS) having fallen two steps at home. years ( 2 ).
Bradykinin Mediated Plasma globulins called kininogens release bradykinin and cause vascular permeability. Image: ( Morgan 2010 ) Features Absence of urticaria and pruritus Insidious onset (24-36 hours) ACE Inhibitors Inhibition of ACE hinders the degradation of bradykinin and can lead to idiosyncratic angioedema.
Date: September 28th, 2021 Reference: Zampieri et al. Date: September 28th, 2021 Reference: Zampieri et al. Some bench work, observational studies, and now two large, unblinded, cluster-randomized single-center trials ( SMART and SALT-ED ) suggested a benefit to using balanced crystalloids (i.e. Reference: Zampieri et al.
These medications are a vital tool in the care of ED patients, from simple local analgesia for a laceration repair to regional analgesia for painful procedures. Metabolism of ester anesthetics is by plasma cholinesterase, whereas amides are metabolized by the cytochrome P450 system in the liver. [6] lidocaine) or an ester (e.g.,
All you know, back in ED, is that the ETA is 10 minutes, and there is a single stab wound to the chest. The ODP is caught up leaving theatres and has not yet made it down to ED. The trauma call goes out. You will be running the show today, and you want to use your preparation time well. to −0.5%]; P = 0.03.). to −0.5%]; P = 0.03.).
Giancarelli et al found that 97% of patients who underwent massive transfusion protocols during trauma resuscitation were hypocalcemic (iCa < 1.1 Kyle et al demonstrated that transfusing a single unit of pRBCs can lead to significant decreases in Ca. How does this impact what you do in the ED? J Trauma Acute Care Surg.
DEG is rapidly absorbed when ingested and can reach peak plasma and brain tissue concentrations within four hours of ingestion. Metabolism of DEG adapted from Bessenhofer, et al. References: Abubukar et al. “Diethylene Glycol” in Goldfrank’s Toxicologic Emergencies , 11e Eds. Nelson, et al.
Case: A 45-year-old woman presents to the emergency department (ED) with itching to bilateral palms. 5 Identification of obstructive physiology in the emergency department (ED) and referral for definitive management can spare patients from these damaging downstream consequences. Her triage vitals are within normal limits.
2,3 Here we examine some of the evidence behind the various components of MTPs, specifically calcium and factor VIIa, and the ratios in which the main products of red blood cells, plasma, and platelets should be administered. Holcomb JB, Tilley BC, Baraniuk S, et al. Cornelius B, Ferrell E, Kilgore P, et al. 2020;88(5):383-9.
Schnapp, MD, MEd (Associate Program Director, University of Wisconsin) // Reviewed by: Joshua Lowe, MD (EM Attending Physician, USAF), Marina Boushra (EM-CCM, Cleveland Clinic Foundation); Brit Long, MD (@long_brit) Case A 36-year-old pregnant woman at 21 weeks gestation presents to the ED with chest pain. N Am J Med Sci. 2014;6(10):491-499.
2 TTP often presents abruptly, and most patients that develop it first visit the emergency department (ED) as their symptoms worsen. 1 Pregnant patients are particularly vulnerable to misdiagnosis of TTP in the ED. References Sukumar S, Lämmle B, et al. Kessler CS, Khan BA, et al. Li XM, Mo XY, et al. J Clin Med.
Moreover, LTOWB also allows us to administer platelets and plasma, in addition to red cells, to promote clotting and homeostasis. If you don't have access to LTOWB and are administering component therapies such as PRBCs or plasma, this is still incredible and I highly encourage it! Minino AM, Heron MP, Murphy SL, et al.
An 18-year-old woman presented to the emergency department (ED) with symptoms of nausea, vomiting, diarrhea, and abdominal pain. Before arriving at our ED, the patient sought care at an urgent care clinic, where she was prescribed ondansetron without improvement. References Katibi OS, Olaosebikan R, et al. Am J Trop Med Hyg.
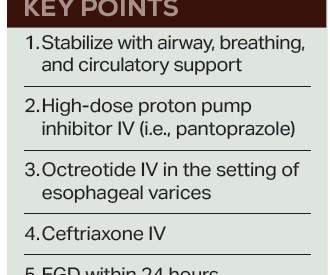
Fresh frozen plasma, or FFP, should only be given to cirrhotic patients as part of the massive transfusion protocol in cases of profound hypotension, as “patients with cirrhosis rarely have true enzymatic hypocoagulability, and FFP may worsen bleeding due to over-resuscitation and dilution of coagulation factors.” 6 Balloon tamponade (i.e.,
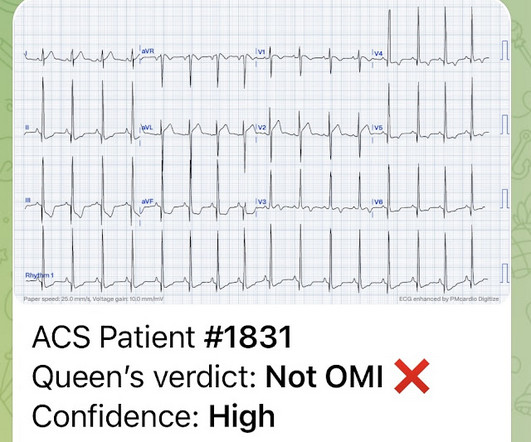
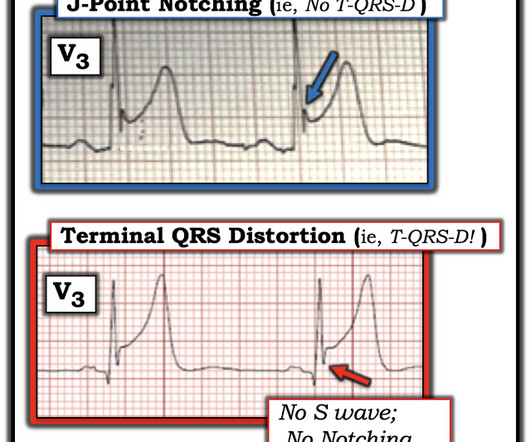
On arrival to the ED, the patient was diaphoretic, tachycardic. I did not think it was due to ACS, but we ordered an ED ECG immediately: What do you think? Peak plasma concentration of amphetamines is rapid ( within minutes ) following inhalation or injection. and had dilated pupils. He was alert and oriented.
Here is his ED ECG: There is obvious infero-posterior STEMI. the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. Internal potassium balance and the control of the plasma potassium concentration. Plasma potassium ([K] p ) was measured at 15-minute intervals during and after the infusion in 31 patients.
They transported to the ED. The history, obtained subsequently, is interesting: The patient had been seen at an outside ED 2 days prior and the K was 2.5 Hospital admission had been recommended, but she left that ED against medical advice. the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al.
In fact, there is laboratory evidence that CO toxicity increases Plateletneutrophil aggregates and plasma myeloperoxidase (MPO) concentration and thus may precipitate ACS (though this is by no means clinically proven). Yelken B et al. Intravascular Neutrophil Activation Due to Carbon Monoxide Poisoning What do you think of this ECG?
This response varies between individuals, age groups and developmental stages, so a single plasma concentration cannot be defined. How do I measure hypoglycaemia in the ED? If there is clinical concern for hypoglycaemia, plasma glucose concentration should be measured. Plasma glucose Beta-hydroxybutyrate (i.e.
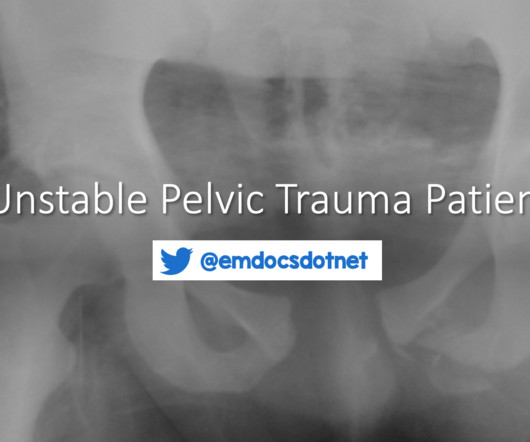
The nuances of fracture patterns and delineating mechanically unstable pelvic fractures from stable ones is less important to the ED. This is less critical in ED management of the unstable pelvic fracture, as the optimal site for identification of rectal or vaginal tears is the operating room.
On arrival to the ED, her blood pressure is 84/36 mmHg with a heart rate of 110 beats per minute. 3,4 Prompt recognition and management of sepsis and septic shock are paramount for the ED clinician. 8,9 Recently, monocyte distribution width (MDW) has shown promise in a large meta-analysis as a useful screening tool in the ED.
F, HR 48, RR 28, BP 104/62, SPO2 88% on non-rebreather mask The patient’s friend who brought her to the ED tells you the patient made suicidal statements earlier in the day and was found in her yard shed. These are send-out labs with turn-around times that make them unlikely to affect the ED course or guide treatment. BMC Res Notes.
These are send-out labs with turn-around times that make them unlikely to affect the ED course. This prevents ongoing exposure to the patient and ED staff. Boostani R, Mellat A, Afshari R, et al: Delayed polyneuropathy in farm sprayers due to chronic low dose pesticide exposure. In: Mattu A and Swadron S, ed. CorePendium.
SCD, therefore, is not only a mechanical disease but there are also many other cellular and plasma factors as well as endothelial interaction that generate chronic inflammation. Haematology specialist clinics are key to manage the chronic side of the disease, while ED doctors should be able to act rapidly on the common acute emergencies.
Treatment requiresaggressive anticoagulation, glucocorticoids, plasma exchange, and intravenous immunoglobulin (IVIG)(27). Aringer M, Costenbader K, Daikh D, et al. Meier AL, Bodmer NS, Wirth C, et al. Tani C, Elefante E, Arnaud L, et al. Bartels CM, Buhr KA, Goldberg JW, et al. 2024;331(17):1480-1491.
A 33-year-old male with a history of drug use presented to the emergency department (ED) for extreme agitation after receiving two doses of 2 mg naloxone by EMS for respiratory depression. If available, an in-house ED pharmacist is an incredible resource for guidance when there are questions regarding pharmacologic management.
In the ED, he develops recurrent respiratory depression and hypoxia to 80%. How long should they stay in the ED? DOI: [link] O’Donnell J, Tanz LJ, Miller KD, et al. Al-Azzawi M, Alshami A, Douedi S, Al-Taei M, Alsaoudi G, Costanzo E. Available at: [link] October 19, 2023 Kelly A, Kerr D, Dietze P, et al.
During observation in the ED the patient had multiple self-terminating runs of Non-Sustained monomorphic Ventricular Tachycardia (NSVT). The minimum effective plasma concentration of flecainide is about 200 ng/mL. This plasma concentration leads to a QRS prolongation of about 10 msec. and Brugada syndrome. Van Zyl, M., &
Louis) // Reviewed by: Joshua Lowe, MD (EM Staff Physician, USAF); Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) Case A 25-year-old woman presented to the emergency department (ED) in Uganda with acute encephalopathy. How is this condition diagnosed and treated in the ED? References Montero DA, Vidal RM, Velasco J, et al.
While this guide isnt exhaustive, its designed by residents, for residents, to provide practical tips and foundational knowledge thats crucial in the fast-paced, high-stakes environment of the ED. Introduction Airway management is a critical ED skill to master. Figure 7: (modified from Tanoubi 2009).
Although the concentration of chloride in the CSF is slightly higher than in plasma, measuring chloride (B) is not an accurate way to detect the presence of CSF. Callen AL, Timpone VM, Schwertner A, Zander D, Grassia F, Lennarson P, Seinfeld J, Lillehei KO, Birlea M, Thaker AA. His left face and eye have severe contusions.
A 51-year-old male with a history of AIDS presents to the ED accompanied by his partner with complaints of cognitive decline and confusion over one month. The development of an inflammatory process is largely due to the infiltration of lymphocytes and plasma cells which ultimately result in nerve damage (e.g., In: StatPearls.
ED Evaluation Transport to the ED from the refugee reception center takes 1 hour. Labs Laboratory workup in the ED is notable for a leukocytosis of 41,000/L, hemoglobin of 6.5 She is sent to the medical ward after three days in the ED with the diagnoses of resolving septic shock, severe malaria, and AKI. 57 Table 2.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content