This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Date: November 22, 2023 Reference: Stopyra et al. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Date: November 22, 2023 Reference: Stopyra et al. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI.
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).
The latest is Langlois-Carbonneau et al. Our data corroborate that immediate management of a patient with a normal automated triage ECG reading is not modified by real-time ED physician ECG interpretation." Smith comment: we showed that the first troponin, even in full-blown STEMI, is negative 25% of the time.
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP).
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. Deutch et al. Fortunately the patient did not reocclude while awaiting the angiogram.
[display_podcast] Date: October 19th, 2017 Reference: Hofmann et al. display_podcast] Date: October 19th, 2017 Reference: Hofmann et al. The ECG shows an inferior ST-Elevated Myocardial Infarction (STEMI). A systematic review by Wijesinge et al from 2009 found only two randomized control trials looking at supplemental oxygen.
BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI. The patient continued to verbalize cessation of symptoms while in the ED.
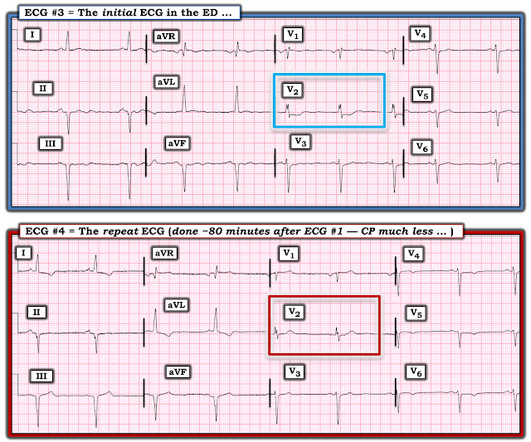
Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al. Patient 1 : anterior OMI Compared with baseline (first ECG), the initial ED ECG (second ECG) has mild ST elevation and hyperacute T waves V2-3 and mild ST depression in V6.
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. The following ECG was captured upon arrival at the receiving ED. The ED resulted an 8.7 Then, three minutes later… Crews activated STEMI as she deteriorated into PEA arrest.
They wanted to know if I would like them to activate the outside hospital's "STEMI alert." But of course, this is not a STEMI by definition as it does not meet STEMI criteria. The STEMI guidelines do state that hyperacute T-waves "may indicate early acute myocardial infarction" but do not discuss it as a "STEMI equivalent."
[link] Case continued She arrived in the ED and here is the first ED ECG. Lindahl et al. From Gue at al. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery.
Here was his initial ED ECG: Formal interpretation by interventional cardiologist: There is "Non-diagnostic" ST Elevation in V2-V4 and aVL. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. 5% vs. 58%!!
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. Below is the initial ED ECG. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. Manual of Cardiovascular Medicine (5th ed.). Smith comment : V5 and V6 are excessively discordant!!!!
He had walked into the ED (did not use EMS). Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Raitt et al.) [and 3) Oliva et al. (3) Armstrong PW et al. Very unlikely.
A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. Here is the final ECG just prior to ED transfer. The attending crews were concerned for an ACS-equivalent of LAD occlusion and initiated a prehospital STEMI activation to the closest PCI center. References 1] Smith, S.
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
Here is his initial ED ECG: What do you think? Here it is: Obvious Inferior Posterior STEMI (+) OMI. Then the ED doc would be dependent on that first ECG. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. Or had not had a prehospital ECG on the ambulance.
He had walked into the ED (did not use EMS). Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Raitt et al.), Raitt et al.), Armstrong et al.),
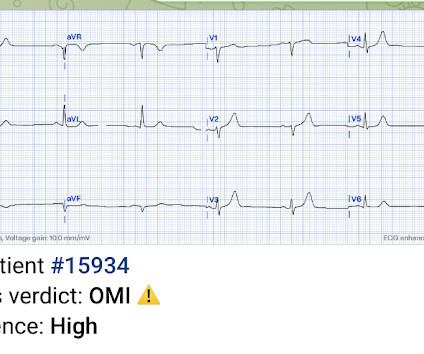
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby Emergency Department where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
A 36 yo male smoker presented to the ED with chest pain. You can see how V1, V2, aVR, and V4R would have ST elevation in either a right ventricular STEMI or with a septal STEMI, and how lateral leads, and even posterior leads, would have reciprocal ST depression. In a 1999 study by Engelen et al. mm at J-point, 2.5
A 61 year-old with chest pain arrived to the ED by ambulance with resolving chest pain. Here is his ED ECG: The computer interpretation was " normal " What do you think? link] Hughes KE et al. The cath lab was activated, as it should be with transient STEMI. This ECG is NOT normal. There is low QRS amplitude.
It was present on arrival at triage but then resolved before bed placement in the ED. Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). Lemkes JS, et al. At times the pain does go to his left neck.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chest pain and RBBB. The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. Do either, both, or neither have occlusion MI? Vitals were normal.
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
The Queen of Hearts agrees: Here the Queen explains why: However, it was not interpreted correctly by the providers: ED interpretation of ECG: "paced rhythm, LBBB but no STEMI pattern." Most large STEMI have peak troponin I in the 20.0 There are hyperacute T-waves in V5 and V6. Next trop in AM. Peak trop 257.97 ng/mL - 80.0
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Herzog et al. Khan et al.
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." In fact, Kosuge et al. Stein et al. This is a paper worth reading : Marchik et al. Kosuge et al. Witting et al. of patients with PE and 3.3% of patients without PE.
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ).
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
There is mixed overlap of ST-segment elevation (STE), ST-segment depression (STD), Hyperacute T waves (HATW), and deWinter pattern (which the ACC regards as a STEMI-equivalent but is better suited under the blanket of OMI). link] [1] Zachary et al. Chou's Electrocardiography in Clinical Practice, 6th ed. 2] Costanzo, L.
The ECG’s were sent to the PCI center, and the providers in the respective ED identified the T wave characteristics mentioned above. STEMI was activated and the patient went to Cath on arrival. Chou’s Electrocardiography in Clinical Practice (6th ed). link] [1] Mirand, D. Canadian Journal of Cardiology, 34 ; 132-145. [2]
Figure 1-1 My colleague, a faithful student of ECG interpretation, handed me the tracing and said that it warranted STEMI activation because of apparent terminal QRS distortion (TQRSD) in V2. ASA 324mg was administered while a STEMI activation was simultaneously transmitted to the nearest PCI center. 4] Baranchuk, A, et al.
He arrived in the ED and had this ECG recorded: There are Wellens' waves, type A (upsloping ST segment then inversion of the terminal part of the T-wave - terminal T-wave inversion, or biphasic T-waves) in V2-V4, and aVL. This male in his 40's had been having intermittent chest pain for one week. Type B waves are deeper and symmetric.
EMS recorded this ECG during active symptoms and transmitted it to the ED: I had no information when I was shown the ECG. I believe there is not quite enough STE for formal STEMI criteria, but some might measure 1.0 I believe there is not quite enough STE for formal STEMI criteria, but some might measure 1.0 Carley et al.
Case history A middle-aged woman with a history of HTN, but no prior CAD, presented to the ED with chest pain. The criteria of Armstrong et al. would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. Can you diagnose an ACO (STEMI) when you also have LVH? One retrospective analysis by Armstrong et al.
ECG 1 at time zero EARLY REPOLARIZATION ABNORMAL ECG ED final official overread: "early repol vs hyperacute T, minimal changes from previous (previous shown below)" What do YOU think? Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Lemkes et al. Is it normal STE? This is a "Transient OMI".
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). He appeared to be in shock.
link] In this paper, in a department in which they state they have only 50 STEMI per year, they looked at only 8 days worth of triage ECGs for a total of 538. They did not find one STEMI on their triage ECGs (no surprise! They only looked at ED diagnosis, not at any angiogram or even at discharge diagnosis. October 2018.
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
Validation of the Modified Sgarbossa Rule for Diagnosis of STEMI in the Presence of Left Bundle Branch Block. His ED ECG showed his baseline LBBB, with no evidence of MI. Meyers HP et al. Pendell is the lead author on our Modified Sgarbossa Criteria Validation Study. Limkakeng AT. Theiling BJ. 0 0 1 41 238 MMRF 1 1 278 14.0
The precordial ST-depression pattern on this ECG (and in this clinical setting) should immediately raise suspicion of Posterior STEMI! Posterior STEMI occurs in approximately 15-20% of acute MI, but the vast majority of the time it is seen in conjunction with inferior (Infero-Posterior) or lateral (Postero-Lateral) STEMI (1).
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. Conversely, Matetzky et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content