This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
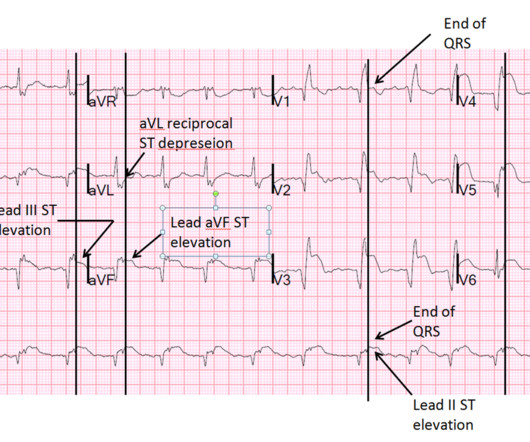
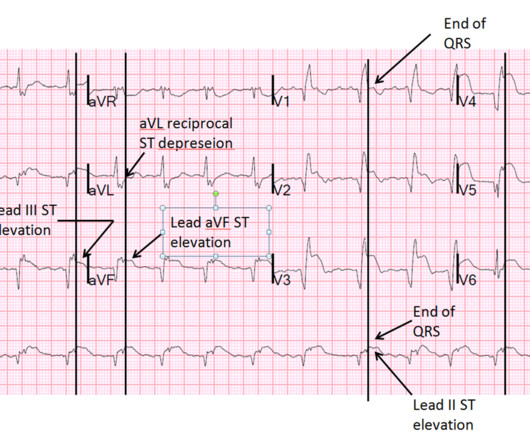
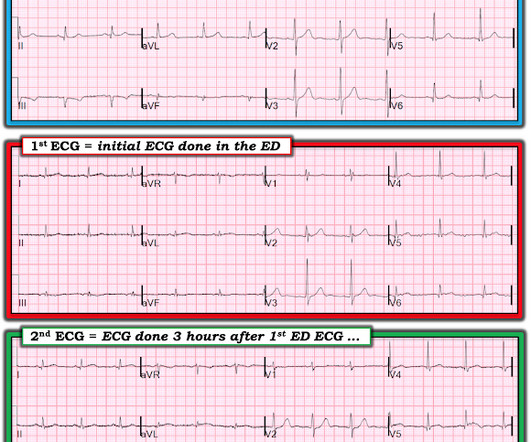
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
Now lets walk through them quickly: Ho et al (4) looked at termination of VT in 15 min or hemodynamic deterioration. Gorgels et al (5) looked at procainamide vs lidocaine and again and primary outcome was VTach termination. Manz et al (6) looked at ajmaline vs lidocaine for the termination of VT. and Komura et al.,
The latest is Langlois-Carbonneau et al. If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management.
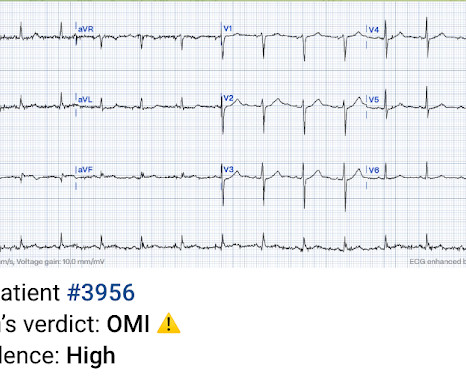
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergencydepartment with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion.
If you were working in a busy emergencydepartment, would you like to be interrupted to interpret these ECGs or can these patients safely wait to be seen because of the normal computer interpretation? have published a number of warnings about the previous reassuring studies.[4,5]
Date: September 8th, 2021 Reference: Desch et al. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. first appeared on The Skeptics Guide to Emergency Medicine. Date: September 8th, 2021 Reference: Desch et al.
Date: January 28th, 2019 Reference: Chu DK et al. Guest Skeptic: Dr. Robert Edmonds is an emergency physician in the US Air Force in Virginia. DISCLAIMER: THE […] The post SGEM#243: Enough is Enough (O2 Saturation of 94-96%) first appeared on The Skeptics Guide to Emergency Medicine. Reference: Chu DK et al.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. In fact, Kosuge et al. Stein et al. This is a paper worth reading : Marchik et al. Kosuge et al.
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
Many conditions outside of acute coronary syndrome (ACS) mimic ST-elevation myocardial infarction (STEMI), but only a handful of cases have reported ST-elevations (STE) in the setting of pancreatic inflammation where underlying ACS was excluded. 2 Proposed hypothesis as described by Hsu et al., Yu ES, Lange JJ, Broor A, et al.
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby EmergencyDepartment where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Raitt et al.) [and Armstrong et al.)], the presence of such well developed anterior Q-wave suggests completed transmural STEMI.
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. New insights into the use of the 12-lead electrocardiogram for diagnosing acute myocardial infarction in the emergencydepartment.
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Raitt et al.), Raitt et al.), Armstrong et al.), 3) Oliva et al. (4) Armstrong PW et al.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergencydepartment with 2 days of heavy substernal chest pain and nausea. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Bigger et al.
There is mixed overlap of ST-segment elevation (STE), ST-segment depression (STD), Hyperacute T waves (HATW), and deWinter pattern (which the ACC regards as a STEMI-equivalent but is better suited under the blanket of OMI). link] [1] Zachary et al. Western Journal of Emergency Medicine, 18 (4), 752-760. [2] 2] Costanzo, L.
Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Lindahl et al. From Gue at al.
Written by Kaley El-Arab MD, edits by Pendell Meyers and Stephen Smith A 61-year-old male with hypertension and hyperlipidemia presented to the emergencydepartment for chest tightness radiating to the back of his neck that has been intermittent for the past day or two. It is true this ECG does not meet STEMI criteria (there is 1.0
Quiz : What percent of full blown STEMI have an open artery with normal flow at angiogram? It too is "normal" and you decide that this is not OMI or STEMI and you just decide to get troponins. Jesse McLaren et al. I would expect that a stent would be placed. In the meantime, a lot of myocardium is lost.
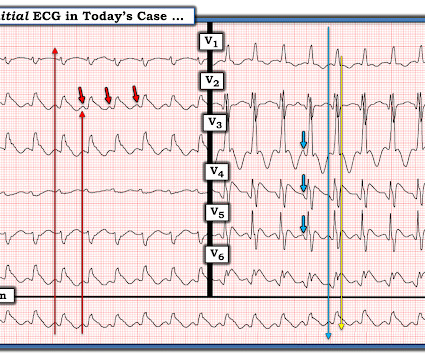
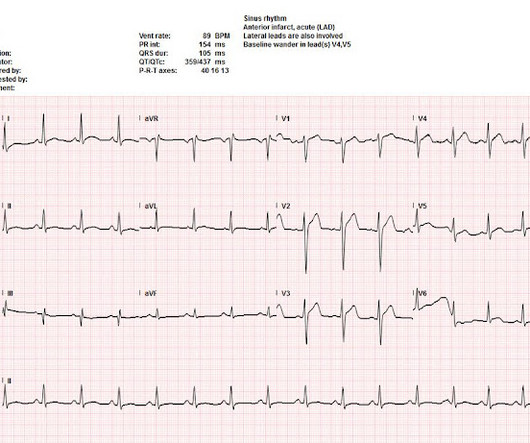
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
STEMI was activated and the patient went to Cath on arrival. New insights into the use of the 12 Lead Electrocardiogram for diagnosing Acute Myocardial Infarction in the emergencydepartment. The distribution of findings is consistent with the LAD, of which is now open with improved TIMI flow. link] [1] Mirand, D. 4] Meyers, H.
STEMI , ST-segment elevation acute myocardial infarction ). 1 Initial diagnosis of STEMI ECG Management Recommendation Level of evidence A 12-lead ECG should be interpreted immediately (within 10 minutes) at first medical contact. I B Designated PCI centres should provide angiography and reperfusion 24/7 without delay.
His ECG was repeated at this point: This shows a well developed anterior STEMI. To not see these findings is very common, and this patient would be given the diagnosis of NonSTEMI, with subsequent development of STEMI. It is not a missed STEMI, but it is a missed coronary occlusion. Fesmire et al. Marti D et al.
It was ongoing on arrival in the emergencydepartment. But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. The emergency physician was called to see the patient 90 minutes later after the troponin I returned at 1100 ng/L. What do you think? Take home 1.
Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Also note that they allow ST depression c/w posterior MI to be a STEMI equivalent. Kurkciyan et al.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergencydepartment with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. New ST elevation diagnostic of STEMI [equation value = 25.3
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
A 35-year-old male presented to the emergencydepartment complaining of chest pain that started 1.5 5 Studies looking at this phenomenon in the emergencydepartment setting for patients presenting with chest pain are lacking. Dr. Young is an emergency physician at Saint Francis Hospital and Medical Center, Hartford, Conn.
Emergency physicians have earned the right to “re-brand” ourselves as indispensable, money-saving change agents in the health care enterprise. Of course, the bill for any episode of emergencydepartment (ED) care can be substantial, exceeding the billed charges for equivalent care provided in some primary care offices.
AslangerE A 65-year-old gentleman presented to the emergencydepartment after experiencing two recent ICD shocks in the preceding hours. As per Dr. Aslanger — a number of medical providers were initial confused by what initially appears as marked ST elevation with reciprocal ST depression, indicative of an acute STEMI.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. Harhash AA, Huang JJ, Reddy S, et al. aVR ST segment elevation: acute STEMI or not?
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the EmergencyDepartment with severe intermittent chest pain. Barely any STE, and thus not meeting STEMI criteria. Only now that the patient has STEMI criteria is he allowed to go to the cath lab, at around 0530.
The remainder of his EmergencyDepartment stay was uneventful. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? Physician interpretation: "No STEMI." Physician: "No STEMI." He had no symptoms of ACS.
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Backus BE, Six AJ, Kelder JC, et al. Am J Emerg Med 2020 3.
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in EmergencyDepartment COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. 3–8 Shi et al. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0 Sandoval Y, Smith SW, Sexter A, et al.
Not seeing any changes on the initial 12 lead ECG, the emergency physician got a 15 lead ECG (below, where V4-6 are actually V4R and V7-8): There’s no posterior ST elevation but the anterior ST depression has resolved between the first and second ECG. Smith : this proves my impression that the inferior T-waves on the first ECG are hyperacute.
Khan AR, Golwala H, Tripathi A, et al. The Smith-Modified Sgarbossa Criteria Accurately Diagnose Acute Coronary Occlusion in EmergencyDepartment Patients With Ventricular Paced Rhythm. BOTTOM LINE: Despite cardiac pacing — ECG #2 is diagnostic of a very large acute anterior STEMI. In normal conduction , (i.e.,
Here is a video lecture of subtle LAD occlusion: One hour lecture on Subtle ECG Findings of Coronary Occlusion The 3-variable formula comes from this paper: Smith SW et al. Annals of Emergency Medicine 2012;60:45-56. These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc A value greater than 22.0
Here is the repeat ECG at 52 minutes after arrival to triage: Obvious posterolateral STEMI Angiographic findings: 1. Reference: • Writing Committee, Kontos MC, de Lemos JA, et al. Comparison of the ST-Elevation Myocardial Infarction (STEMI) vs. NSTEMI and Occlusion MI (OMI) vs. NOMI Paradigms of Acute MI. Meyers HP, Smith SW.
I do research on Cardiologs' algorithm: Smith SW et al. A Deep Neural Network learning algorithm outperforms a conventional algorithm for emergencydepartment electrocardiogram interpretation. Peguero JG et al. But lead V2 has a worrisome amount of ST elevation, and in a chest pain patient, I would be worried about STEMI.
PCI mid LCx So this is an OMI (Occlusion Myocardial Infarction), but not a STEMI Echo: Decreased left ventricular systolic performance, mild/moderate. Sandoval Y et al. This figure comes from the Diamond T study (all type 1 MI were NSTEMI, not STEMI): Notice that the 6 hour value (far right) is very low for type 2 MI.
STEMI negative : the EMS automated interpretation read, “STEMI negative. According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. Sinus bradycardia.”
Written by Pendell Meyers A man in his late 30s with history of hypertension, tobacco use, and obesity presented to the EmergencyDepartment for acute chest pain which started approximately 3 hours prior to arrival, in the setting of a very stressful situation. de Winter et al in N Engl J Med 359:2071-2073, 2008.
A middle aged patient who was 3 weeks s/p STEMI came from cardiac rehab where he developed some chest pain, dyspnea and weakness on the treadmill. There is no acute STEMI. This is diagnostic of recent, reperfused STEMI. This is diagnostic of recent, reperfused STEMI. Acute STEMI would have upright T-waves.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content