This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Date: November 22, 2023 Reference: Stopyra et al. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Date: November 22, 2023 Reference: Stopyra et al. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI.
Now lets walk through them quickly: Ho et al (4) looked at termination of VT in 15 min or hemodynamic deterioration. Gorgels et al (5) looked at procainamide vs lidocaine and again and primary outcome was VTach termination. Manz et al (6) looked at ajmaline vs lidocaine for the termination of VT. Coolest part of this trial?
Date: September 8th, 2021 Reference: Desch et al. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. Date: September 8th, 2021 Reference: Desch et al. The TOMAHAWK Investigators. The TOMAHAWK Investigators.
Written by Jesse McLaren A previously healthy 60 year old developed exertional chest pain with diaphoresis, and called EMS. Here’s the EMS ECG, digitized with PM cardio. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
EMS was called, and they recorded the following ECG on scene at 13:16: What do you think? In this medical system, the EMS provider can then be routed to the ED or to a type of urgent care facility that is open 24 hrs/day and staffed by a primary care provider. In this case, the EMS provider was routed to the urgent care facility.
According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. It’s important to stress the presence of a normal QRS (i.e.,
Written by Pendell Meyers I received this prehospital ECG (we receive prehospital ECGs by telemetry from EMS in a large area around our hospital) and was told that there was a patient in her 50s with chest pain who was headed to an outside hospital (which happens to be a catheterization center). Here is the ECG: What do you think?
Fire/EMS personnel find her laying supine on the kitchen floor, awake and verbal, although acutely ill. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. Wolters-Kluwer: Philadelphia, PA.
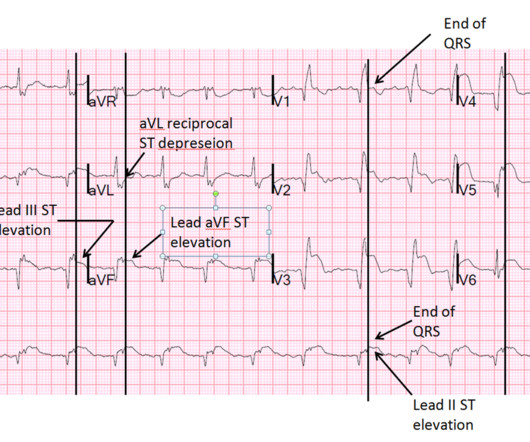
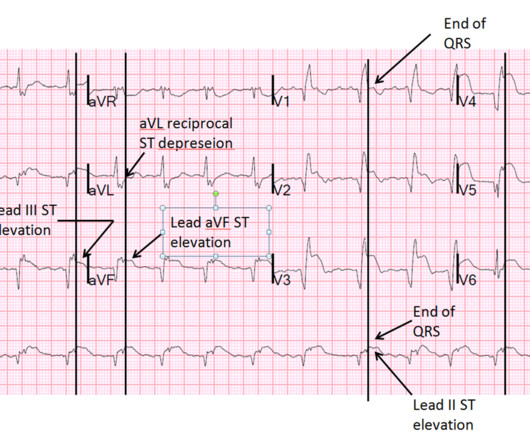
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
He presented to EMS with extreme pallor, Levine sign, diaphoresis, bilateral arm pain, and an apprehensive sense of doom. link] [1] Zachary et al. David Didlake, NRP, APRN, ACNP-BC This case is provided by C. Madden, Paramedic. Many thanks for sharing! Past medical history included HTN, HLD, and MI 10 years prior. 2] Costanzo, L.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Vitals were normal except for oxygen saturation of 94%.
When EMS found her, she was dyspneic and diaphoretic. The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. She was out walking her dog when she developed sudden dizziness and light-headedness.
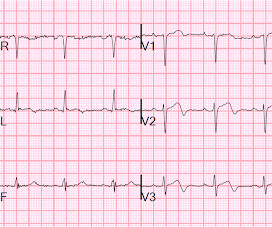
EMS arrived and recorded this ECG: What do you think? Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case.
Written by Pendell Meyers A middle aged man called EMS for acute chest pain. EMS recorded this ECG during active symptoms and transmitted it to the ED: I had no information when I was shown the ECG. I believe there is not quite enough STE for formal STEMI criteria, but some might measure 1.0 Carley et al. Tandberg et al.
Figure 1-1 My colleague, a faithful student of ECG interpretation, handed me the tracing and said that it warranted STEMI activation because of apparent terminal QRS distortion (TQRSD) in V2. ASA 324mg was administered while a STEMI activation was simultaneously transmitted to the nearest PCI center. 4] Baranchuk, A, et al.
The case below was contributed by Pendell Meyers, an EM G1 at Mt. Validation of the Modified Sgarbossa Rule for Diagnosis of STEMI in the Presence of Left Bundle Branch Block. Meyers HP et al. Sinai (the case did not come from Mt. Sinai though!) Pendell is the lead author on our Modified Sgarbossa Criteria Validation Study.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 Akkerhuis KM, et al. Gottlieb SO, et al. Jernberg T, et al. Patel DJ, et al.
EMS obtained the following vital signs: pulse 50, respiratory rate 16, blood pressure 96/49. It appears EMS obtained two EKGs, but unfortunately these were not saved in the medical record. The EMS crew was only BLS certified, so EKG interpretation is not within their scope of practice.
Article Summary by Sarah Fabiano, MD, FACEP, FAAEM Lyng JW, Braithwaite S, Abraham H, et al. Appropriate air medical services utilization and recommendations for integration of air medical services resources into the EMS system of care: a joint position statement and resource document of NAEMSP, ACEP, and AMPA.
He awoke from sleep with crushing central chest pain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. This male in his 40's had been having intermittent chest pain for one week. Type B waves are deeper and symmetric. A stent was placed. de Zwaan C., Janssen J.H.A., de Zwaan C.,
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chest pain. Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. Is this OMI? Today’s Post by Dr.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al.
Emergency medicine (EM) has evolved over time and has long passed a crossroads where previously unachievable capabilities should be celebrated and shared. Gulati M, et al. Stiell IG, et al. Stiell IG, et al. Hoffman JR, et al. Stiell IG, et al. Schonfeld D, et al. Stiell IG, et al.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). Hayakawa A, Tsukahara K, Miyagawa S, et al. He was diagnosed as NSTEMI. He had already been given aspirin and heparin.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. What do you see?
This is an extremely important topic especially for EMS systems that are implementing High Performance CPR , because it is very predictable that you are going to see a lot more patients with return of pulses in the field, and if you don’t have a plan, lots of things can go wrong before arriving at the hospital. Thanks for joining us.
This post was written by Tarissa Lai, one of our outstanding EM residents at Hennepin County Medical Center, with comments by Steve Smith and Dan Lee. female with HTN, HLD, diabetes, ESRD on dialysis is brought in by EMS with sudden onset, left -sided chest pain for the past four hours. Case A 30 something y.o.
The patient had this ECG recorded at 7 minutes after registration at triage as a walk-in (not by EMS): What do you think? Here is the repeat ECG at 52 minutes after arrival to triage: Obvious posterolateral STEMI Angiographic findings: 1. Reference: • Writing Committee, Kontos MC, de Lemos JA, et al. Here is the case in total.
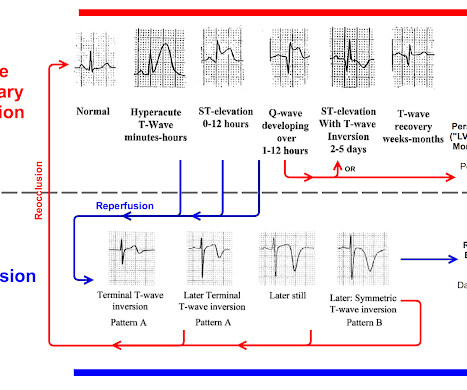
Failure to do so may result in overlooking subtle ST-T wave changes in a patient "in passage" from a frank STEMI toward reperfusion changes. POINT #2: The initial tracing in today's case does not show acute changes.
Background: Primary PCI is the recommended reperfusion strategy in patients with STEMI and should be initiated within 2 hours after first medical contact. Paper: Van de Werf, F et al. In non-PCI-capable hospitals this goal is not always achievable due to delays in transfer. Primary PCI: 95.7% Primary PCI: 95.7% Primary PCI: 78.4%
Written by Jesse McLaren A 75 year old with a history of CABG called EMS after 24 hours of chest pain. STEMI negative : the EMS automated interpretation read, “STEMI negative. Even if the patient had presented acutely with STEMI criteria, the ST elevation resolved on arrival though the pain continued.
He reported to EMS a medical history of GERD only. BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI. However, in this context (i.e.
About 2 hours later the patient arrived at a PCI-capable center and repeat ECG was obtained: The transferring EMS crew noted “runs of VT” during transport. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Bigger et al. Is there STEMI? Leave it alone. Moffat, M.
He had walked into the ED (did not use EMS). Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Raitt et al.) [and 3) Oliva et al. (3) Armstrong PW et al. Very unlikely.
He had walked into the ED (did not use EMS). Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Raitt et al.), Raitt et al.), Armstrong et al.),
link] Hughes KE et al. PMID: 27519772 This recent study, discussed on Salim Rezaie's fine site REBEL EM , implies you can trust the computer interpretation of "normal." ( [link] ) What to do? The cath lab was activated, as it should be with transient STEMI. It is not yet available, but this is your way to get on the list.
EMS found her acutely ill, mottled, dry mucous membranes, modestly hypotensive, and lethargic. The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. Example 1 EMS is called to the residence of an elderly male experiencing profound weakness.
This guideline revision is particularly timely as EMS systems have shown their abilities to dramatically improve survival and neurologic outcome after cardiac arrest, STEMI, acute stroke, and other time-sensitive conditions. References Lulla A, et al. Spaite DW, Bobrow BJ, Keim SM, et al. Prehosp Emerg Care. J Safety Res.
STEMI was activated and the patient went to Cath on arrival. The distribution of findings is consistent with the LAD, of which is now open with improved TIMI flow. The ECG’s were sent to the PCI center, and the providers in the respective ED identified the T wave characteristics mentioned above. link] [1] Mirand, D. 2] Aslanger, E.,
This is by one of our outstanding 3rd year residents , Aaron Robinson, with some edits and comments by Smith EMS responded to a reported seizure in a 42 year old male. One of our EMS Fellows along with a Senior EM Resident were on duty that evening, and arrived on the scene with the Fire Department. Why is the patient in shock?
Zeymer HT et al. References: Zeymer HT et al. PMID: 37634145 Post Peer Reviewed By: Anand Swaminathan, MD (Twitter/X: @EMSwami ) The post The ECLS-SHOCK Trial: ECPR in Infarct-Related Cardiogenic Shock appeared first on REBEL EM - Emergency Medicine Blog. bleeding, stroke, limb ischemia, and hemolysis). Control: 53.4%
The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chest pain. The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. The pain was 10/10 in intensity radiating bilaterally to the shoulders and also to the left arm and neck. The below ECG was recorded.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content