This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Epinephrine and cardiac arrest: what’s the question? How much epinephrine is enough? Garcia et al. published a retrospective study in AJEM discussing cumulative epinephrine dosage in cardiac arrest.
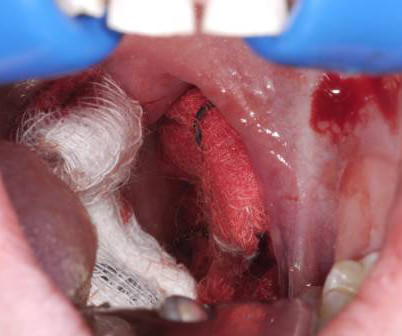
6 Apply direct pressure to the bleeding site with gauze soaked in TXA and epinephrine as a first-line intervention. 7 Epinephrine acts as a local vasoconstrictor, aiding hemostasis, and TXA helps to stabilize clot formation on the exposed tissue and delay hemorrhage progression. References Grasl S, Mekhail P, Janik S, et al.
Reference: Snyder BD, Van Dyke MR, Walker RG, et al. Reference: Snyder BD, Van Dyke MR, Walker RG, et al. Association of small adult ventilation bags with return of spontaneous circulation in out of hospital cardiac arrest. Resuscitation 2023. Resuscitation 2023.
Date: September 18, 2024 Reference: Dillon et al. You and your partner initiate high-quality CPR, place a supraglottic airway, establish intra-osseous (IO) access and administer epinephrine. Reference: Dillon et al. Naloxone and Patient Outcomes in Out-of-Hospital Cardiac Arrests in California. JAMA Network Open.
Both norepinephrine and epinephrine can be used. Epinephrine is key if there is significant bradycardia. Tenenbein M, Macias CG, Sharieff GQ, et al, eds. Tenenbein M, Macias CG, Sharieff GQ, et al, eds. Crystalloid may help, but neurogenic shock may not respond to fluid administration. References Coleman-Satterfield, TT.
Date: December 6th , 2018 Reference: Perkins et al. A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. Date: December 6th , 2018 Reference: Perkins et al. A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. JAMA 2009, Hagihara et al. JAMA 2012 and Cournoyer et al.
How Long Should We Monitor After Giving IM Epinephrine for Anaphylaxis? Bottom Line Up Top: After prompt recognition and appropriate treatment with IM epinephrine, the risk of biphasic reactions are exceedingly low. At the time of discharge, appropriate patient education and prescriptions for IM epinephrine are essential.
” Reference: Vallentin et al. Intraosseous access is quickly obtained, and a dose of epinephrine is provided. Reference: Vallentin et al. Effect of Intravenous or Intraosseous Calcium vs Saline on Return of Spontaneous Circulation in Adults With Out-of-Hospital Cardiac Arrest – A Randomized Clinical Trial.
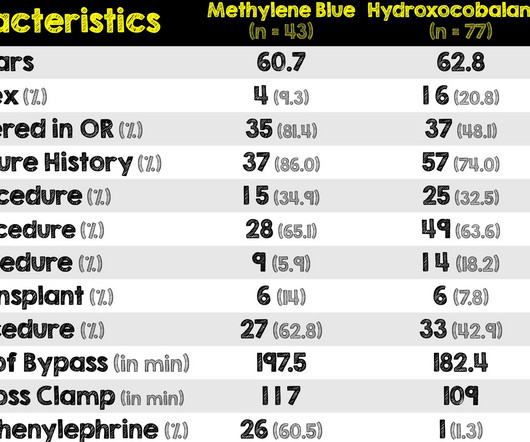
1-4 The PDPs, phenylephrine and epinephrine, result in vasoconstriction and increased cardiac contractility. They can be associated with side effects such as reflex bradycardia, decreased stroke volume in phenylephrine, tachycardia and hypertension associated with epinephrine. Paper: Singer S, et al. Am J Emerg Med. 2022 Sep 5.
Date: October 18th, 2022 Reference: Moore et al. Date: October 18th, 2022 Reference: Moore et al. This includes epinephrine for OHCA, target temperature management, mechanical CPR, supraglottic airways, steroids, hands on defibrillation and many more topics. first appeared on The Skeptics Guide to Emergency Medicine.
Most emergency drugs except for amiodarone and succinylcholine are based on ideal body weight [Emergency Medical Services for Children, Luten 2007] Epinephrine, dopamine, fentanyl, ketamine based on what child should weigh. link] Lubitz DS, Seidel JS, Chameides L, Luten RC, Zaritsky AL, Campbell FW. and Seaver, M. Rosenberg, M.S.
Reference: Vent et al. Buffered lidocaine 1%, epinephrine 1:100,000 with sodium bicarbonate (hydrogencarbonate) in a 3:1 ratio is less painful than a 9:1 ratio: A double-blind, randomized, placebo-controlled, crossover trial. . Epinephrine in Local Anesthetics: This will not make the tip of things fall off (nose, fingers, toes, etc).
Date: February 7, 2023 Reference: Cheskes et al. Date: February 7, 2023 Reference: Cheskes et al. Reference: Cheskes et al. Defibrillation Strategies for Refractory Ventricular Fibrillation. first appeared on The Skeptics Guide to Emergency Medicine. Defibrillation Strategies for Refractory Ventricular Fibrillation.
Date: November 10th, 2021 Reference: Andersen, et al: Effect of Vasopressin and Methylprednisolone vs Placebo on Return of Spontaneous Circulation in Patients With In-Hospital Cardiac Arrest. Epinephrine is provided and you quickly place an advanced airway. JAMA Sept 2021. JAMA Sept 2021. The monitor shows a non-shockable rhythm.
[display_podcast] Date: September 19th, 2017 Reference: Cournoyer et al. display_podcast] Date: September 19th, 2017 Reference: Cournoyer et al. There have been a number of papers published since OPALS that support the findings of not using ACLS drugs like epinephrine for OHCA: * Olavseengen et al. September 2017.
Date: January 5th, 2021 Reference: Grunau et al. Date: January 5th, 2021 Reference: Grunau et al. This has included things like therapeutic hypothermia ( SGEM#54 , SGEM#82 , SGEM#183 and SGEM#275 ), supraglottic devices ( SGEM#247 ), crowd sourcing CPR ( SGEM#143 and SGEM#306 ), and epinephrine ( SGEM#238 ).
[display_podcast] Date: September 12th, 2017 Reference: Sinert et al. display_podcast] Date: September 12th, 2017 Reference: Sinert et al. epinephrine, histamine blockers, corticosteroids) the underlying mechanism of action predicts that these medications will not work. Reference: Sinert et al.
[display_podcast] Date: September 21st, 2018 Reference: Kawano et al. display_podcast] Date: September 21st, 2018 Reference: Kawano et al. As part of their protocol, they attempt vascular access to administer epinephrine and an antidysrhythmic. EMS arrives on scene and initiates high quality basic life support (BLS).
A study by Lee et al ( 7) compared femoral CVC placement to IO and demonstrated a first-pass success pass rate with IO of 90.3% In cardiac arrest, a delay in IV access subsequently results in a delay in epinephrine administration. References: 1 Astasio-Picado Á et al. Ong MEH, Chan YH, Oh JJ, et al. Iserson KV et al.
Reference: Cashen K, Reeder RW, Ahmed T, et al. Reference: Cashen K, Reeder RW, Ahmed T, et al. 1] The SGEM has covered the use of epinephrine, vasopressin, methylprednisolone, and calcium for cardiac arrest in SGEM#238 , SGEM#350 , and SGEM#353. Pediatric Crit Care Med. Pediatric Crit Care Med.
Read More EMCrit: Podcast 145 – Awake Intubation Lecture from SMACC ERCast: Angioedema References: Baş M et al. PMID 25629740 Hassen GW et al. PMID 23062323 Kostis JB et al. PMID 16043683 McCormick M et al. PMID 20954277 Sinnert R et al. Zuraw et al. N Engl J Med. 2015; 372(5):418-25. 2013;24:53-66.
2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. 5 More recent literature defines “refractory” as VT or VF that is persistent or recurrent despite three shocks from a defibrillator, three rounds of epinephrine, and use of an antiarrhythmic (i.e.,
[display_podcast] Date: June 20th, 2017 Reference: Bernard et al. display_podcast] Date: June 20th, 2017 Reference: Bernard et al. They continue CPR, get intravenous access, give a round of epinephrine and then wonder if they should start rapid cooling en-route to the hospital with some cold saline. Reference: Bernard et al.
SGEM#317: Dese bones gonna heal again, with or without a non-selective NSAID Reference: George et al. SGEM Bottom Line: There is no high-quality evidence to support the claim that non-selective NSAIDS cause an increased risk of nonunion. Risk of Nonunion with Nonselective NSAIDs, COX-2 Inhibitors, and Opioids. J Bone Joint Surg Am.
Disease-Oriented Outcomes (DOOs) The PARAMEDIC-2 trial looked at the effectiveness of epinephrine in adult patients who suffered an out-of-hospital cardiac arrest. They found that epinephrine administration was associated with higher survival at 30 days ( 3.2% doi:10.1136/bmjebm-2018-110891 Perkins GD, Ji C, Deakin CD, et al.
Traditional Advanced Cardiovascular Life Support (ACLS) medications, namely epinephrine, have been known to exacerbate coronary vasospasm. References Prinzmetal M, Kennamer R, Merliss R, et al. Myerburg RJ, Kessler KM, Mallon SM et al. Magid DJ, Aziz K, Cheng A, et al. Kousik SM, Graves SM, Napier TC, et al.
1,2] Consider using a physiological marker to help identify inadvertent vascular injection, such as epinephrine. [3] If epinephrine is used, small initial doses ( <1 ug/kg) are preferred. doi:10.1136/bcr-2019-233119 Neal JM, Barrington MJ, Fettiplace MR, et al. 5,8] In one review the incidence of LAST was estimated to be 2.7
Dell KM, et al. Eisen S et al. Fielder AR, et al. Bm MV, et al. Toepfner N, et al. Toniutti M, et al. Meoli M, et al. Ashton JJ, et al. Ding G et al. Tanti DC, et al. Ahlqvist VH, et al. Chiang HL, et al. Wong J, et al. Fuller S et al. Koenis MM et al.
Paper: Hiruy A, et al. to 1mg/kg/hr) Information regarding the vasopressors used in the study is as follows: Norepinephrine equivalents = norepinephrine mcg/kg/min + (phenylephrine mcg/kg/min/10) + epinephrine mcg/kg/min + (vasopressin units/min x2.5) REFERENCES: Hiruy A, et al. PMID: 37586951 Mehaffey JH, et al.
Paper: Vallentin MF et al. References: Vallentin MF et al. Additionally, there were non-statistically significant trends toward lower survival and lower survival with good neurologic outcomes in patients receiving calcium at 30 to 90 days. It is unknown whether these harms are present at long-term follow up. Resus 2022. Placebo: 9.1%
1] The Adult Cardiac Arrest ACLS algorithm currently includes epinephrine and either amiodarone or lidocaine as recommended pharmacologic therapies. al answered this question with a prospective observational study which showed a significantly shorter time interval to obtain tibial IO access (4.6 1] Table from Hamam et al.
Multiple attempts at defibrillation, epinephrine, and amiodarone have been unsuccessful. References Go AS, Mozaffarian D, Roger VL, et al. Larribau R, Deham H, Niquille M, et al. Margey R, Browne L, Murphy E, et al. Kudenchuk PJ, Brown SP, Daya M, et al. Spies DM, Kiekenap J, Rupp D, et al. Circulation.
The data in the paper by Rangel et al. Lange RA, Cigarroa RG, Flores ED, et al. McCord J, Jneid H, Hollander JE, et al. Esmolol in the management of epinephrine- and cocaine-induced cardiovascular toxicity. is intuitive, and not surprising. style='mso-element:field-begin'> ADDIN EN.CITE Rangel 1853 1853 17 Rangel, C.
When simple maneuvers fail, we proceed to topical agents such as lidocaine with epinephrine, oxymetazoline, anterior nasal packing, and electrical or chemical cauterization. Paper: Zahed R, Moharamzadeh P, Alizadeharasi S et al. Initial interventions include local pressure, ice, and forward head positioning for persistent bleeds.
When simple maneuvers fail, we proceed to topical agents such as lidocaine with epinephrine, oxymetazoline, anterior nasal packing, and electrical or chemical cauterization. Paper: Zahed R, Moharamzadeh P, Alizadeharasi S et al. Initial interventions include local pressure, ice, and forward head positioning for persistent bleeds.
Some look promising (ie eCPR and application of US) while others have been considerably less effective or inconsistent (ie epinephrine and targeted temperature management). Article: Moore JC et al. References: Moore JC et al. Additionally, there is ongoing research into targeting improvements in the interventions we know work.
After several cycles of defibrillation, epinephrine, and amiodarone, the patient remains in cardiac arrest. Current AHA guidelines do not recommend routine use of calcium in cardiac arrest (Panchal, et al., Calcium acts as a vasopressor and inotropic agent (Lindqwister, et al., He is found to be in ventricular fibrillation (VF).
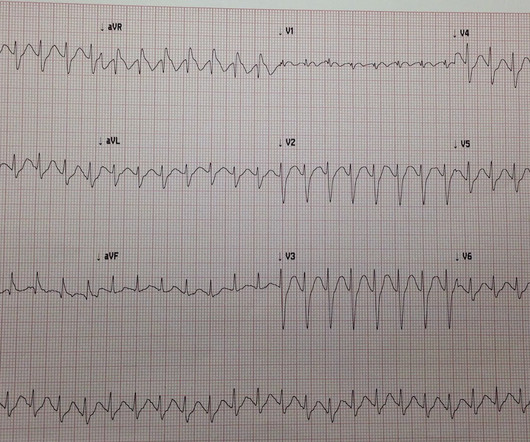
Fine ventricular fibrillation She received 2 mg epinephrine, 150 mg amiodarone and underwent chest compressions with the LUCAS device. She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. see below). I have never seen this, but it is possible.
Casey The CLOVERS trial: National Heart, Lung, and Blood Institute Prevention and Early Treatment of Acute Lung Injury Clinical Trials Network; Shapiro NI, Douglas IS, Brower RG, et al. Epinephrine metered-dose inhaler for pediatric croup. Early Restrictive or Liberal Fluid Management for Sepsis-Induced Hypotension. N Engl J Med.
Article: Abella BS et al. Zuberbier, Torsten, et al. Moreover, the FDA approved intravenous (IV) cetirizine to treat acute urticaria in 2019. Clinical Question: Is IV cetirizine noninferior to IV diphenhydramine for the treatment of acute urticaria? Ann Emerg Med 2020. J Allergy Clin Immunol. 2004 Feb;113(2):347-52. PMID: 14767453.
Dobutamine may be preferred in patients without severe hypotension who have high vascular resistance. -- De Backer D et al. Taglieri N, Marzocchi A, Saia F, et al. Kosuge M, Ebina T, Hibi K, et al. Richard, C; et al. Safian RD, Berman AD, Diver DJ, et al. Hutter AM Jr, De Sanctis RW, Nathan MJ, et al.
REBEL Cast Ep113 – Defibrillation Strategies for Refractory Ventricular Fibrillation Click here for Direct Download of the Podcast Paper: Cheskes S, et al. REFERENCES: Cheskes S, et al. 2022 Nov 6 PMID: 36342151 Cheskes S, et al. Defibrillation Strategies for Refractory Ventricular Fibrillation. N Engl J Med. N Engl J Med.
Epinephrine administered intravenously. After 13 minutes of ALS resuscitation, pulses were palpated indicating a return of spontaneous circulation. They administered 10 mcg of push-dose epinephrine. Atropine and further doses of epinephrine were not administered. Approach TCP with skepticism.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content