This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
HIET improves contractility without increasing SVR, while vasopressin and epinephrine transiently increase SVR/MAP but worsen cardiac output in anesthetized dogs given propranolol (Holger 2007). Disposition to ICU. References: Yuan TH, Kerns WP, Tomaszewski CA, et al. von Lewinski D, Bruns S, Walther S, et al.
Reference: Cashen K, Reeder RW, Ahmed T, et al. Sodium bicarbonate use during pediatric cardiopulmonary resuscitation: a secondary analysis of the icu-resuscitation project trial. Reference: Cashen K, Reeder RW, Ahmed T, et al. Background: We often manage patients in cardiac arrest in the ED or the intensive care unit (ICU).
1-4 The PDPs, phenylephrine and epinephrine, result in vasoconstriction and increased cardiac contractility. They can be associated with side effects such as reflex bradycardia, decreased stroke volume in phenylephrine, tachycardia and hypertension associated with epinephrine. Paper: Singer S, et al. Am J Emerg Med. 2022 Sep 5.
Paper: Ibarra-Estrada, M et al. What They Did: Single-center, parallel, double blind, randomized controlled trial performed in a medical-surgical ICU (Mexico) Both groups received: Adjunctive vasopressin initiated at a dose of 0.03 Limited, small studies on its use in septic shock do not make a clear argument for use. Crit Care 2023.
1,2] Consider using a physiological marker to help identify inadvertent vascular injection, such as epinephrine. [3] If epinephrine is used, small initial doses ( <1 ug/kg) are preferred. Hemodynamics slowly begin to stabilize, and the patient is transferred to the ICU for further post-cardiac arrest care. BMJ Case Rep.
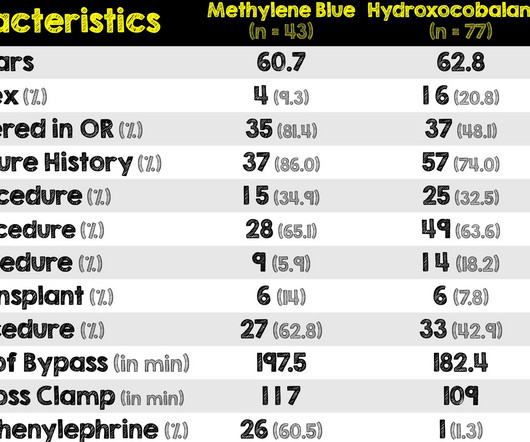
Paper: Hiruy A, et al. to 1mg/kg/hr) Information regarding the vasopressors used in the study is as follows: Norepinephrine equivalents = norepinephrine mcg/kg/min + (phenylephrine mcg/kg/min/10) + epinephrine mcg/kg/min + (vasopressin units/min x2.5) REFERENCES: Hiruy A, et al. PMID: 37586951 Mehaffey JH, et al.
The patient received 1 mg of epinephrine IV x2 with conversion of his rhythm to ventricular fibrillation (VF) for which he was defibrillated twice in the field. He requires low-dose epinephrine to maintain his mean arterial pressure (MAP) in the 60s mmHg and is transported to the cardiothoracic (CT) ICU. Carsten L, et al.
Article: Kumar M et al. The TEG group had a shorter ICU length of stay in the first admission. Patients exclusively managed in the ICU which decreases applicability for patients in other locations Very small sample size of 96 patients No definition was provided for exclusion criteria of significant cardiopulmonary disease.
Nielsen N, Wetterslev J, Cronberg T et al. By the time of the study by Nielsen et al. Kirkegaard H, Soreide E, de Haas, I et al. Kirkegaard et al. De Fazio C, Skrifvars MB, Soreide E et al. Targeted temperature management at 33°C versus 36°C after cardiac arrest. New Engl J Med. 2013;369(23):2197–2206.
Below follows a drug manual for use in the CCU (coronary care unit), ICU (intensive care unit) or ER (emergency room). Epinephrine Shock (any) Cardiac arrest Bronchospasm Anaphylaxis Bradycardia (second-line alternative) Infusion : 0.01 References Overgaard, Dzavik et al. Jentzer et al. Increases coronary blood flow.
Atchinson PRA, Hatton CJ, Roginski MA, et al. Ittrich H, Bockhorn M, Klose H, et al. Li H, Ding X, Zhai S, et al. Kathuria H, Hollingsworth HM, Vilvendhan R, et al. Fekri MS, Hashemi-Bajgani SM, Shafahi A, et al. Wand O, Guber E, Guber A, et al. O‘Neil ER, Schmees LR, Resendiz K, et al. BMC Pulm Med.
34 If a MAP of 65 mmHg is still not achieved, epinephrine should be added as a third agent (Figure 1). For patients with septic shock and cardiac dysfunction that are persistently hypotensive, it is appropriate to use norepinephrine and dobutamine or epinephrine alone. References Evans L, Rhodes A, Alhazzani W, et al.
He was started appropriately on vancomycin and cefepime and accepted for ICU admission but remains in the ED due to boarding and bed lock. Left ventricular outflow tract obstruction in ICU patients. doi:10.1016/S0033-0620(05)80036-2 Balik M, Novotny A, Suk D, et al. doi:10.3390/JCM13185344 Yamagishi T, Tanabe T, Fujita H, et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content