This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Major adverse cardiac events 40 minutes after giving the antiarrhythmic. The following table shows their results, take a look: Note that procainamide leads with less adverse cardiac events. Procainamide therapy was associated with less major cardiac adverse events and a higher proportion of tachycardia termination within 40 min.
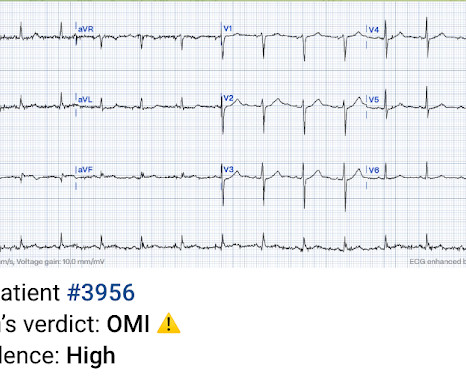
This was a machine read STEMI positive OMI. 118.007305) from Heitner et al. , The meaning of this quote is that at times, something as obvious as the dramatic anterior lead ST elevation that we see in today's tracing is not the result of an acute LAD STEMI. His ECG is shown below. Pretty obvious anterior current of injury.
Even in patients whose moderate stenosis undergoes thrombosis, most angiograms show greater than 50% stenosis after the event. Lindahl et al. See "Prevention of cardiovascular disease events in those with established disease (secondary prevention) or at very high risk".) From Gue at al.
COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. Lemkes JS, Janssens GN, van der Hoeven NW, et al. These physicians did not want a patient with an OMI that was not a STEMI to be randomized to no angiogram.
They wanted to know if I would like them to activate the outside hospital's "STEMI alert." But of course, this is not a STEMI by definition as it does not meet STEMI criteria. The STEMI guidelines do state that hyperacute T-waves "may indicate early acute myocardial infarction" but do not discuss it as a "STEMI equivalent."
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. Deutch et al. Fortunately the patient did not reocclude while awaiting the angiogram.
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published.
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
Quiz : What percent of full blown STEMI have an open artery with normal flow at angiogram? It too is "normal" and you decide that this is not OMI or STEMI and you just decide to get troponins. Jesse McLaren et al. I would expect that a stent would be placed. In the meantime, a lot of myocardium is lost.
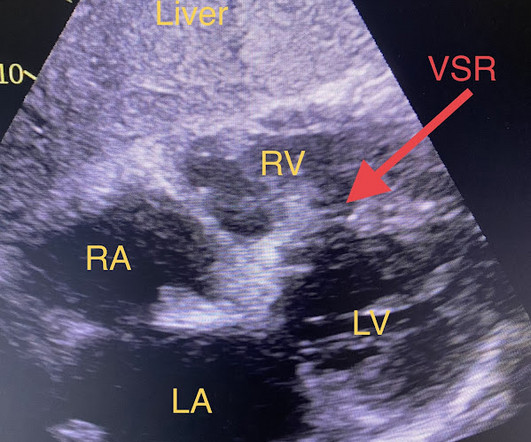
A Short Comment on PIRP and T Waves: Oliva et al found a strong association of myocardial rupture with postinfarction regional pericarditis. It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI.
Here it is: Obvious Inferior Posterior STEMI (+) OMI. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.) The cath lab was activated prehospital But imagine if the patient had walked in.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. He was started on nitro gtt.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Herzog et al. Khan et al. Circulation 2007 2.
Troponin T peaked at 2074 ng/L (very high, typical of OMI/STEMI). As a result — the onset of any acute event that may have occurred is uncertain. Post PCI the patient became gravely hypotensive and "shocky". She stabilized on dobutamine and levosimendan infusions that could be discontinued after 24 hours. 21, 2017 ).
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Lemkes JS, et al.
Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Lemkes et al. And dynamic ST-T wave changes between ECG #1 and ECG #2 confirm an acute event in progress. Is it normal STE?
Figure 1-1 My colleague, a faithful student of ECG interpretation, handed me the tracing and said that it warranted STEMI activation because of apparent terminal QRS distortion (TQRSD) in V2. Whether this represents a potential acute cardiac event would depend on the history, comparison with prior tracings and serial tracings.
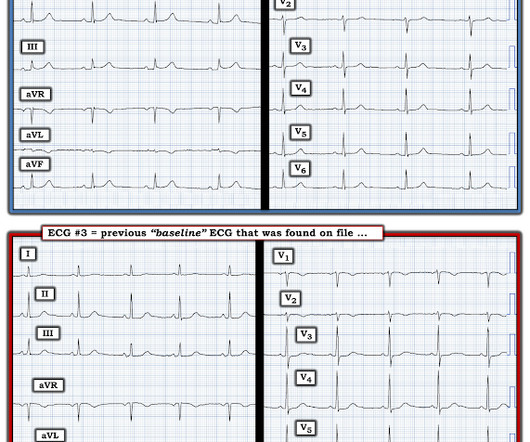
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. In the largest study looking at this topic by Mizusawa et al., She has not had a heart catheterization or after this event so the presence or absence of CAD is still unknown.
The criteria of Armstrong et al. would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. The physician was concerned about STEMI, but also worried that she was overreacting, with the potential that LVH was producing a "STEMI-mimic." Can you diagnose an ACO (STEMI) when you also have LVH?
Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." And Olivier finishes with this commentary: "Yet another example in favor of abandoning STEMI criteria for diagnosing OMI. Peak troponin: 128,000 ng/L.
Heitner et al. We also know that initial ECG(s) may be non-diagnostic despite a recent event ( ie, IF an acute occlusion spontaneously opens after only a brief period of time — or if the initial ECG is obtained during the "pseudo-normalization" period ). The PDA plaque was also bulky, but was not described as inflamed or ulcerated.
STEMI , ST-segment elevation acute myocardial infarction ). 1 Initial diagnosis of STEMI ECG Management Recommendation Level of evidence A 12-lead ECG should be interpreted immediately (within 10 minutes) at first medical contact. I C If possible, patients should bypass non-PCI centres to a PCI-capable centre.
That's because this patient has clinical, ECG and Troponin evidence that an acute event did in fact occur ( ie, a more than doubling of Troponin in the context of a changing pattern of CP that correlates temporally with "dynamic" ECG changes — therefore strongly suggesting transient acute occlusion regardless of cath findings in today's case ).
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. Thelin et al. Mokhtari et al. These include: i ) appreciation of how problematic the definition of “acute STEMI” can be; and , ii ) illustration of how dependence on this definition may result in overlooking acute coronary occlusion.
You may have mastered all the latest changes affecting management of sepsis, STEMI, and opiate-use disorder, but there’s no stopping the relentless revisions to our approach to neurologic emergencies. The authors report an excess bleeding events in the tenecteplase cohort, likely leading to the neutral effect on overall survival.
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 Akkerhuis KM, et al. Gottlieb SO, et al. Jernberg T, et al. Patel DJ, et al.
Prognosis from brain injury results not only from the initial or primary injury, but also from secondary injury that occurs after the event, mainly, hypoxic/ischemic brain injury from under resuscitation or cerebral edema from the release of neurotoxic inflammatory mediators. References Lulla A, et al. Prehosp Emerg Care. J Safety Res.
Barely any STE, and thus not meeting STEMI criteria. Annals of Emergency Medicine Cardiology was called to evaluate the patient immediately for emergent cath, but they stated that the ECG did not meet STEMI criteria and elected to wait for further information before proceeding with cath. He was given 6mg IV morphine for ongoing pain.
Takotsubo is a sudden event, not one with crescendo angina. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Even in patients whose moderate stenosis undergoes thrombosis, most angiograms show greater than 50% stenosis after the event. Lindahl et al.
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Backus BE, Six AJ, Kelder JC, et al. Moumneh T, Sun BC, Baecker A, et al.
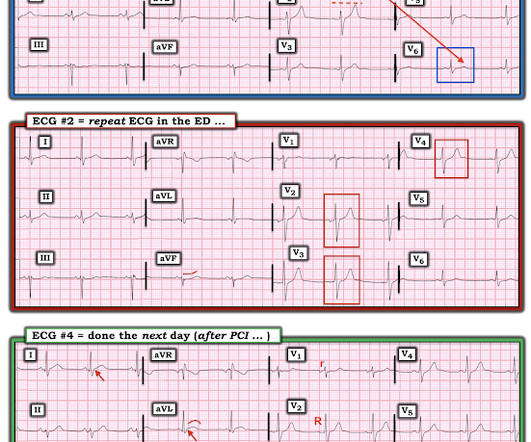
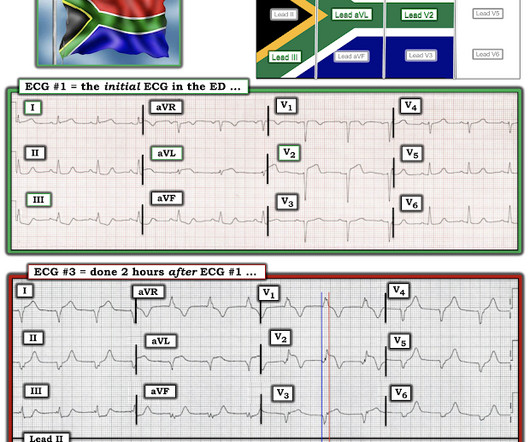
While not essential for making the "correct clinical decision" ( which would have been prompt cath performed much sooner than it was ) — I thought serial ECGs did reveal important clues to the ongoing event. Figure-1: I've labeled the 1st, 2nd and 4th tracings in today's case ( See text ).
A recent study found that SCAD causes almost 20% of STEMI in young women. A study by Hassan et al. Lobo et al. examined SCAD presenting as STEMI (unlike Hassan et al. Lobo et al. examined SCAD presenting as STEMI (unlike Hassan et al. The SCAD cases in Lobo et al.
50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. 24 yo woman with chest pain: Is this STEMI? This is not "diffuse", this is simply anterior, lateral, and likely apical.
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? Physician interpretation: "No STEMI." Physician: "No STEMI." Cardiologist interpretation: "Technically does not meet STEMI criteria but concerning for ischemia."
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. In the largest study looking at this topic by Mizusawa et al., Bicarb 20, Lactate 4.2, Ammonia 100.
Considering hyperacute T-waves have been accepted as STEMI equivalents, it is possible that pseudonormalization could gain more recognition as an indicator of ACS. Sequence of events in angina at rest: Primary reduction in coronary flow. References Noble RJ, Rothbaum DA, Knoebel SB, McHenry PL, Anderson GJ. Arch Intern Med.
3–8 Shi et al. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0 Sandoval Y, Smith SW, Sexter A, et al. Shi S, Qin M, Shen B, et al.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). Hayakawa A, Tsukahara K, Miyagawa S, et al. Am J Emerg Med. 2014;32:e5–e8. J Cardiol Cases. 2022;25(6):404-407. 2022.01.006 6.
There is clearly sufficient STE for STEMI criteria in leads V2 and aVL, but lead I has less than 1.0 mm of STE - thus, technically this ECG does not meet STEMI criteria, although it is a quite obvious OMI. This ECG was immediatel y discussed with the on-call cardiologist who said the ECG was "concerning but not a STEMI."
There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI). In fact, the STE is widespread, mimicking an anterior STEMI. See this paper by Smith et al.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. Taglieri N, Marzocchi A, Saia F, et al. Kosuge M, Ebina T, Hibi K, et al. What do you see?
These findings are very subtle but suspicious for LAD occlusion, as we have seen in many similar (but less difficult) cases on this blog: A man in his sixties with chest pain at midnight with undetectable troponin How long would you like to wait for your Occlusion MI to show a STEMI? Learning Points: Not all OMI will present as STEMIs.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content