This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
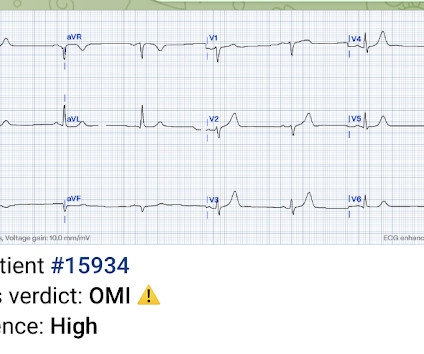
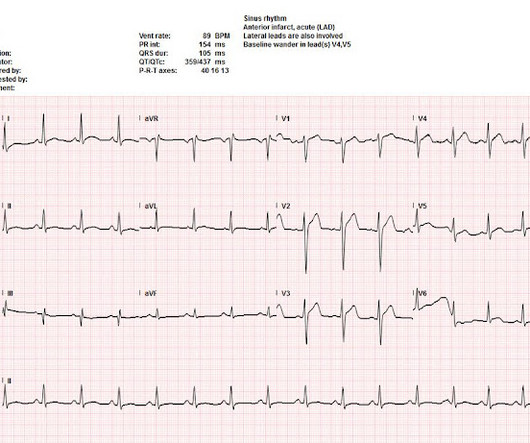
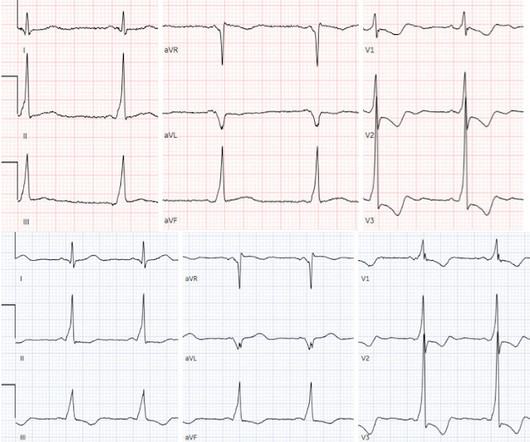
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
Lets look at a few and make an informed decision. Now lets walk through them quickly: Ho et al (4) looked at termination of VT in 15 min or hemodynamic deterioration. Gorgels et al (5) looked at procainamide vs lidocaine and again and primary outcome was VTach termination. His initial EKG is the following: What do you think?
[display_podcast] Date: October 19th, 2017 Reference: Hofmann et al. display_podcast] Date: October 19th, 2017 Reference: Hofmann et al. The ECG shows an inferior ST-Elevated Myocardial Infarction (STEMI). A systematic review by Wijesinge et al from 2009 found only two randomized control trials looking at supplemental oxygen.
Unknown algorithm The Queen gets it right Case 4 How unreliable are computer algorithms in the Diagnosis of STEMI? The patient's prehospital ECG showed that there was massive STEMI and these are hyperacute T-waves "on the way down" as they normalize. Pain was resolving. Diagnosed as Normal by the computer. Troponin negative.
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. Deutch et al. Fortunately the patient did not reocclude while awaiting the angiogram.
Date: February 1, 2023 Reference: Wolfrum et al. Date: February 1, 2023 Reference: Wolfrum et al. A post-arrest ECG doesn’t show any signs of STEMI. For more information on the fragility index (FI) click on this LINK. Temperature Control After In-Hospital Cardiac Arrest: A Randomized Clinical Trial. Circulation.
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
Lindahl et al. Optical coherence tomography, due to its high resolution, may provide additional information [ 10,13 ]. From Gue at al. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery.
The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Learning points: Both patients and other medical providers can report confusing and often contradictory information that obfuscates the diagnosis (in this case, WPW). Bigger et al. Is there STEMI? Do not treat AIVR.
The chest pain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Learning Points: 1.
Any ST Depression Maximal in V1-V4 is OMI until proven otherwise I sent this ECG with no information to Pendell. Here it is: Obvious Inferior Posterior STEMI (+) OMI. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. We send each other EKG by the dozens every day.
He sent it to me with no other information and I wrote back "100% diagnostic of LBBB with inferior-posterior-lateral OMI" There is atrial paced rhythm with Left Bundle Branch Block (LBBB). Most large STEMI have peak troponin I in the 20.0 This ECG was recorded and was reviewed remotely by a cardiologist: What do you think? 2021;23:187.
If this EKG were handed to you to screen from triage without any clinical information, what would you think? for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." In fact, Kosuge et al. Stein et al. Kosuge et al. Witting et al.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Vitals were normal except for oxygen saturation of 94%. Vitals were normal.
Zeymer HT et al. We don’t know any of this information unfortunately and all are key in patient selection The median lactate level before revascularization was 6.9mmol/L (Range 4.6 References: Zeymer HT et al. The benefits of this strategy may be outweighed by the risk of the device-related complications (i.e. Control: 53.4%
EMS recorded this ECG during active symptoms and transmitted it to the ED: I had no information when I was shown the ECG. I believe there is not quite enough STE for formal STEMI criteria, but some might measure 1.0 I believe there is not quite enough STE for formal STEMI criteria, but some might measure 1.0 Carley et al.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. In such cases — radiofrequency ablation of ectopic beats triggering malignant ventricular arrhythmias was needed for control of arrhythmic storm because the antiarrhythmic medications tried were ineffective ( Marrouche et al — JACC 5;43(9): 1715-20, 2004 ).
You can read this post here, or watch a video presentation of it: [link] I was handed this ECG, without any clinical information, while on my way to see another patient: There is sinus rhythm. If there are no changes in aVL, it is highly unlikely to be inferior STEMI. Would you be certain that it is not STEMI? Tikkanen et al.
I want all to know that, with the right mind preparation, and the use of the early repol/LAD occlusion formula, extremely subtle coronary occlusion can be detected prospectively, with no other information than the ECG. His ECG was repeated at this point: This shows a well developed anterior STEMI. Fesmire et al.
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
Is this an anterior STEMI with LBBB? Explanation : The patient had a worrisome history: 59 yo with significant substernal chest pressure, so his pretest probability of MI (and even of STEMI) is reasonably high. Additionally, appropriate discordance is common in NonSTEMI, but very unusual in coronary occlusion (STEMI).
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. Harhash AA, Huang JJ, Reddy S, et al. aVR ST segment elevation: acute STEMI or not?
Barely any STE, and thus not meeting STEMI criteria. Annals of Emergency Medicine Cardiology was called to evaluate the patient immediately for emergent cath, but they stated that the ECG did not meet STEMI criteria and elected to wait for further information before proceeding with cath. His initial troponin T returned at 0.03
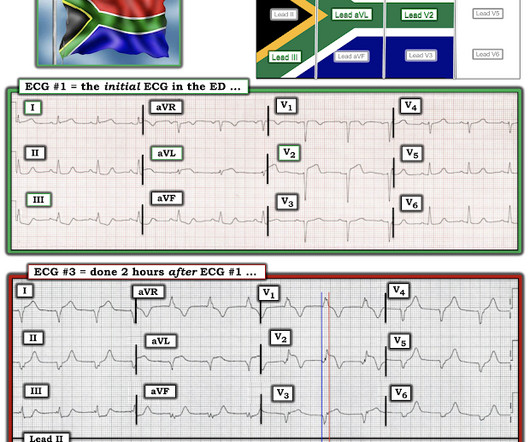
I don't have any clinical information or any other associated ECGs on this case, but wanted to post it here because it is interesting and it is pathognomonic. de Winter et al in N Engl J Med 359:2071-2073, 2008. BOTTOM LINE: ECG #1 does not satisfy criteria for a “STEMI” — because there is not enough ST elevation. What is it?
I sent this "normal" ECG without any information to a number of ECG enthusiasts, who were all concerned about possible OMI - whether subtle high lateral OMI with inferior reciprocal change, or subtle inferior OMI with high lateral reciprocal change. So this was transient STEMI(-)OMI, not transient STEMI.
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? greater than 40mS, V1-V2" Meyers interpretation: I was sent this ECG with no clinical information whatsoever, and I responded: "Easily diagnostic of acute LAD occlusion."
Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Lindahl et al. Optical coherence tomography, due to its high resolution, may provide additional information [ 10,13 ]. From Gue at al. This has resulted in an under-representation of STEMI MINOCA patients in the literature.
3–8 Shi et al. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0 Sandoval Y, Smith SW, Sexter A, et al. Shi S, Qin M, Shen B, et al.
50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. This was sent to me with no information and I immediately replied that it was diagnostic of LAD OMI. Pericarditis?
Smith : without any further information, my interpretation adds that there are inferior hyperacute T-waves and possibly also in V4-V6, and subtle reciprocal ST depression and T-wave inversion in aVL. There’s normal sinus rhythm, normal conduction, normal axis, normal R wave progression, and normal voltages.
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Backus BE, Six AJ, Kelder JC, et al. Moumneh T, Sun BC, Baecker A, et al.
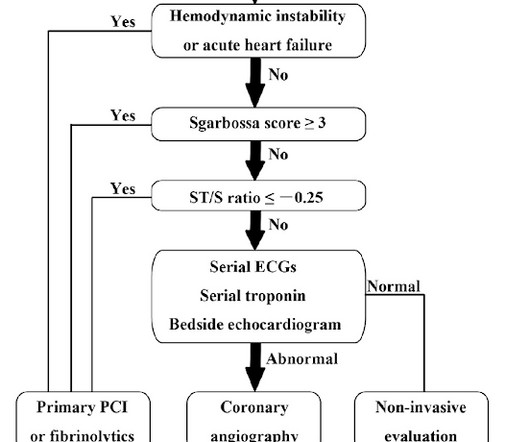
The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. Accordingly, in the algorithm by Cai et al for patients with LBBB and ischemic symptoms ( See below ) — the first indication for PCI is clinical: patients with hemodynamic instability or acute heart failure. Learning points 1.
Here is a video lecture of subtle LAD occlusion: One hour lecture on Subtle ECG Findings of Coronary Occlusion The 3-variable formula comes from this paper: Smith SW et al. These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc The 4-variable formula is based on this paper: Driver, BE et al.
There is clearly sufficient STE for STEMI criteria in leads V2 and aVL, but lead I has less than 1.0 mm of STE - thus, technically this ECG does not meet STEMI criteria, although it is a quite obvious OMI. This ECG was immediatel y discussed with the on-call cardiologist who said the ECG was "concerning but not a STEMI."
Without seeing the patient, my interpretation of the first ECG was: likely normal variant ST-elevation (early repolarization), with a small possibility of pericarditis, and almost no possibility of acute coronary occlusion (STEMI). and therefore highly unlikely to be STEMI. in V6 and J-point notching.
Background Information: Multiple illness severity scores have been developed for use after out-of-hospital cardiac arrest (OHCA) and in-hospital cardiac arrest (IHCA). Unfortunately, these rely on information that is not immediately available to providers in the early hours following return of spontaneous circulation (ROSC).
I sent this to Pendell without any information at all, and he replied "Postero-lateral Reperfusion." Here is the repeat ECG at 52 minutes after arrival to triage: Obvious posterolateral STEMI Angiographic findings: 1. Reference: • Writing Committee, Kontos MC, de Lemos JA, et al. This is a trick question, as you will see below.
Meyers : This ECG was texted to me with no clinical information, and my response was: "That looks like a very subtle LAD OMI. Learning Points: Not all OMI will present as STEMIs. B OTTOM L ine : While ECG #1 does not satisfy the definition of a STEMI — as per Dr. Meyers, it really looks like a cute L AD O MI.
I sent this to Dr. Meyers without any other information, and he responded, “do you have a prior to make sure that it is all just because of the delta wave? But it doesn’t meet STEMI criteria, and was not identified by the computer or the over-reading cardiologist. Rosner et al. What do you think? What do you think? Goldberger.
Written by Pendell Meyers I was reading ECGs in a database (without any clinical information) when I came to this one: What do you think? For clarity in Figure-1 — I've reproduced the initial ECG that was shown above in today's case, which Dr. Meyers ventured to read without the benefit of any clinical information.
Evaluate and treat seizures or SE after CA in the context of other available clinical information because other systemic factors may influence the occurrence of seizures or SE and the effectiveness of treatment (90%, 18/20). Reference: Hirsch KG, Abella BS, Amorim E, et al; American Heart Association, Neurocritical Care Society.
We hosted the inaugural South Carolina Resuscitation Academy April 29-30 on Hilton Head Island, which was very successful, but some of the feedback we received from our attendees was that they would have liked to receive more information about our post-resuscitation care checklist. References Callaway C, Donnino M, Fink E et al.
However, this additional information was supportive. Patients like her are the reason we are advocating for a change in the ACS paradigm from STEMI to OMI. Armstrong et al attempted to study it but may have included too many 'obvious' cases - the criteria from that paper would certainly have missed this case.
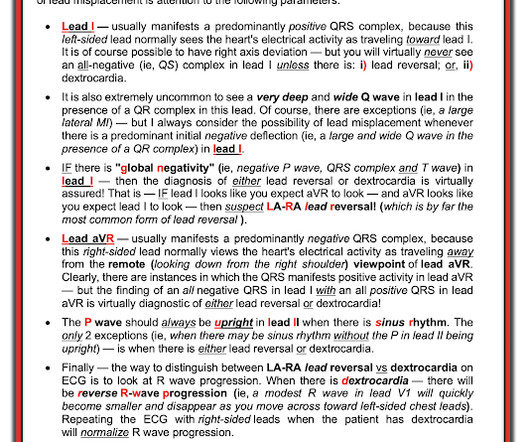
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". Hyperkalemia mimics STEMI and OMI in many distributions, but probably the most common is the Brugada morphology in V1-V2 which mimics anterior OMI for those who cannot recognize the Brugada pattern. Limb lead reversal can be easily recognized.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content