This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
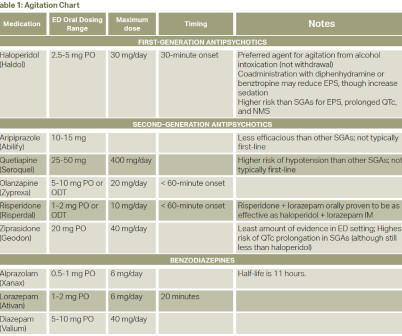
Questions: What are the symptoms of second-generation antipsychotic overdose? How is second-generation antipsychotic overdose diagnosed? What is the treatment for patients who have overdosed on second-generation antipsychotics? 4 The specific incidence of second-generation antipsychotic drug overdose is unknown, however, 4.7%
Background: An update to our 2015 post on HIET for beta-adrenergic receptor and calcium channel antagonists overdose. Beta-adrenergic receptor antagonists (Beta blockers, BB) and calcium channel antagonists (calcium channel blockers) are common drugs that can produce profound cardiac depression and shock when taken in overdose.
Date: September 18, 2024 Reference: Dillon et al. Naloxone is a well-established medication used primarily for reversing opioid overdoses. Traditionally, naloxone has been used in cases of suspected opioid overdose where patients exhibit signs of severe respiratory depression or loss of consciousness (LOC). JAMA Network Open.
Date: June 16, 2023 Reference: Reed et al. Date: June 16, 2023 Reference: Reed et al. EDs are an important touch point for individuals with opioid use disorder (OUD), given the number of encounters for overdose and complications associated with drug use. Reference: Reed et al. AEM June 2023 Guest Skeptic: Dr. .
Recently, xylazine has gained attention in the media with increasing reports of xylazine-related overdose deaths in patients. When combined with illicit opioids such as heroin and fentanyl, xylazine may increase the risk of fatal overdose given the augmented sedation and respiratory depression effects [2]. MMWR Morb Mortal Wkly Rep.
Date: January 17th , 2019 Reference: Clemency et al. Date: January 17th , 2019 Reference: Clemency et al. The EMS crew observes drug paraphernalia and suspect an intravenous (IV) opioid overdose. 1] Two-thirds of the all the drug overdoses in the US in 2016 (63,632) involved an opioid (42,249). [2]
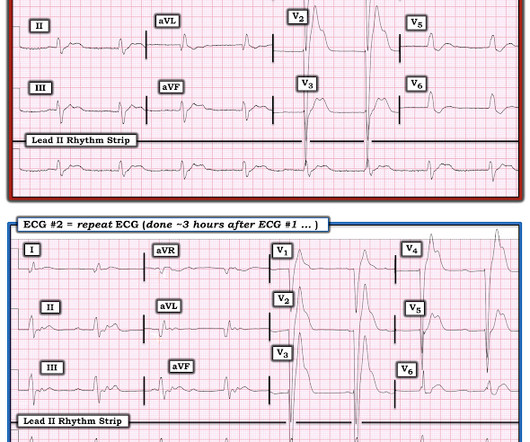
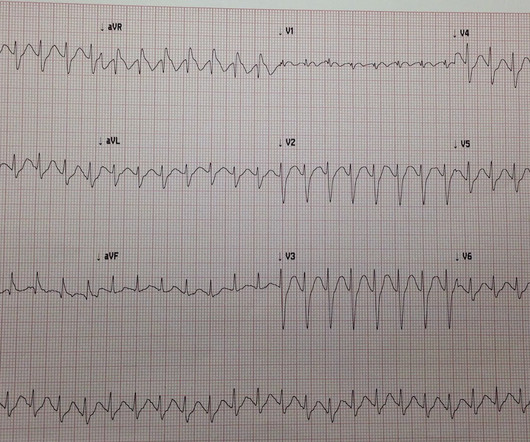
A 20-something presented after a huge verapamil overdose in cardiogenic shock. And she does not know that this is an overdose; she thinks it is a patient with chest pain!! Comment on High Dose Insulin and Calcium Channel Blocker Overdose I do not have any explanation for the ST-T abnormalities here. The initial K was 3.0
[display_podcast] Date: May 19th, 2017 Reference: Willman et al. Do heroin overdose patients require observation after receiving naloxone? display_podcast] Date: May 19th, 2017 Reference: Willman et al. Do heroin overdose patients require observation after receiving naloxone? Reference: Willman et al.
A clinical decision tool called the STUMBL score was derived and validated by Battle et al in 2014 [3]. An attempt was made to externally validate this tool in New Zealand by Murkerji et al 2021 [4]. These risks are particularly higher in the elderly [2]. It risks stratified older patients with blunt trauma.
Reference Lin M, Phipps M, Chan TM, et al. Digital Impact Factor: A Quality Index for Educational Blogs and Podcasts in Emergency Medicine and Critical Care.
Broselow-Luten System: Supportive Data Physician estimates of weight can underdose children by 49% or overdose by up to 116%. link] Lubitz DS, Seidel JS, Chameides L, Luten RC, Zaritsky AL, Campbell FW. 2012.05.028 Silvagni D, Baggio L, Mazzi C, et al. doi:10.1111/1742-6723.12389 Zhu S, Zhu J, Zhou H, et al. Zaritsky, A.,
Xylazine is a veterinary sedative that has been increasingly implicated in overdose deaths throughout the United States. percent of all overdose deaths in 2020. 1 Known by street names such as “tranq,” “tranq-dope,” or “zombie drug,” xylazine is increasingly found in patients with opioid overdose. References Friedman J, et al.
Date: August 23rd, 2022 Reference: Schoenfeld et al. Date: August 23rd, 2022 Reference: Schoenfeld et al. Case: A 24-year-old male presents to the emergency department (ED) after a fentanyl overdose. Reference: Schoenfeld et al. He is successfully resuscitated using naloxone and is stable after an observation period.
What is the difference between ALS and BLS Medical Care? In Advanced Life support (ALS) emergencies, a “single” paramedic or ER doctor can not deliver necessary care. And it becomes impossible to treat multi-system injuries, such as doing chest compression (CPR) while trying to open an airway or control bleeding.
Background Information: Opioid overdose deaths have been increasing in the past twenty years. The national number of overdose deaths from any opioid has increased 62.5% In addition, buprenorphine has a lower risk of death from overdose when compared to methadone (2). Characteristics: Mean age 35.5 Homeless: 32.6%
Opioid overdose remains the leading cause of cardiac arrest due to poisoning in North America. For a patient with suspected opioid overdose who has a definite pulse but no normal breathing or only gasping (ie, a respiratory arrest), in addition to providing standard BLS and/or ALS care, it is reasonable for responders to administer naloxone.
Massive acetaminophen overdose: effect of hemodialysis on acetaminophen and acetylcysteine kinetics. Bebarta VS, Kao L, Froberg B, et al. A multicenter comparison of the safety of oral versus intravenous acetylcysteine for treatment of acetaminophen overdose [published correction appears in Clin Toxicol (Phila). PMID: 27118496.
What are the treatment options for a benzonatate overdose? 7) Overdose literature review timeline: In 1986, the first two benzonatate fatalities were reported in the literature: a choking infant and an intentional overdose in a teenager. (8) There is no specific toxidrome or antidote for a benzonatate overdose.
Right as you’re making your bunk you get dispatched for a reported overdose with police enroute, no further information. We go into it with preconceptions of what to expect: “It’s a simple heroin overdose, we’ll wake them up and they’ll refuse, then we’ll go back to bed”. Iolascon A, Andolfo I, Russo R, et al. Hemasphere.
Click here for Direct Download of the Podcast Paper: Bouzat P et al. References: Bouzat P et al. PMID: 36942533 Innerhofer P et al. PMID: 28457980 Jehan F et al. PMID: 29664892 Zeeshan M et al. High-quality studies are needed to determine the utility of this intervention. Lancet Haematol 2017.
Unfortunately, most cases are not so simple, with half of them being unintentional overdoses, many with a delayed presentation; some with delayed-release formulations, combined formulations, or co-ingestions, and some in patients with co-morbidities—all factors that make recognition and management more challenging. for death. for death.
As it turns out, common sense likely rules the day when presented with patients whose low GCS is the result of a self-limited overdose toxidrome. References Gibbs KW, Semler MW, Driver BE, et al. Luo Z, Li Y, Li W, et al. Knack SKS, Scott N, Driver BE, et al. Escobar GJ, Liu VX, Schuler A, et al. N Engl J Med.
Sometimes this can be used to our advantage, like when we need to give subcutaneous fluids to a dehydrated patient without an IV, or when we need to give SQ medications for things like Sulfonylurea overdose , Hereditary Angioedema , or DVTs. Shen 2013, Nickerson 2014, Scolaro 2016 ] Singh et al proposed an algorithm to guide treatment.
Elimination half-life data is not well established but increases in larger overdoses and as renal injury begins to occur. Metabolism of DEG adapted from Bessenhofer, et al. References: Abubukar et al. Nelson, et al. Conklin, Laura, et al. Nelson, et al. CDC’s Morbidity and Mortality Weekly Report.
In our case, the patient had accidentally overdosed on drugs prior to being found. Carsten L, et al. Monika BM, Martin D, Balthasar E, et al. Forti A, Brugnaro P, Rauch S, et al. 2018.09.018 Romlin BS, Winberg H, Janson M, et al. Klein LR, Huelster J, Adil U, et al. The management of accidental hypothermia.
In such cases — radiofrequency ablation of ectopic beats triggering malignant ventricular arrhythmias was needed for control of arrhythmic storm because the antiarrhythmic medications tried were ineffective ( Marrouche et al — JACC 5;43(9): 1715-20, 2004 ). The most common side effects of Quinidine is hypotension and QTc prolongation.
doi:10.1016/0002-9343(89)90302-1 Guglielminotti J, Pascal Pernet, Maury É, et al. Negative anion gap and elevated osmolar gap due to lithium overdose. 061057 Wu AHB, McKay C, Broussard LA, et al. Ann Am Thorac Soc. 2014;11(4):671-674. doi:10.1513/annalsats.201401-033cc 201401-033cc Weisberg LS. Pseudohyponatremia: A reappraisal.
Click here for Direct Download of the Podcast Paper: Knack SKS et al. References: Knack SKS et al. It is possible that the induction agent used could play an important role on hemodynamic effects in critically ill adults. REBEL Cast Ep120: Etomidate vs Ketamine for RSI in the ED? Range 5 to 9) Etomidate: 7.0 Range 5 to 9) Diff -0.2;
Current AHA guidelines do not recommend routine use of calcium in cardiac arrest (Panchal, et al., Calcium acts as a vasopressor and inotropic agent (Lindqwister, et al., risk ratio >1) was 4% for ROSC, 6% for 30 day survival, and 4% for survival with a favorable neurologic outcome at 30 days (Vallentin, et al.,
Paper: Vallentin MF et al. Although the results of both the short and long-term outcomes of the COCA trial do not support the use of calcium in all patients with OHCA, there are some populations that may still benefit from this treatment including patients with hyperkalemia, hypocalcemia, and calcium channel blocker overdose.
Confounders to the GCS such as seizure and post-ictal phase, ingestions and drug overdose, as well as medications administered in the prehospital setting that impact GCS score should be documented. References Lulla A, et al. Spaite DW, Bobrow BJ, Keim SM, et al. Prehosp Emerg Care. Accessed 2022, [link]. J Safety Res.
There are many underlying causes, such as stroke, central nervous system depression (opioid overdose, etc.), Hopkins, Erin, et al. For the purposes of this discussion, we’ll stick to the four basic types: o Respiratory acidosis results from inadequate alveolar ventilation leading to increased CO2 retention in the bloodstream.
3 When administered early after overdose, nicotinamide may decrease the severity of toxicity. doi: 10.1056/NEJM198001103020202 Buonvicino D, Mazzola F, Zamporlini F, et al. Activated charcoal can be used to prevent absorption in acute ingestions, presenting within an hour of exposure. A clinical study of 12 cases. N Engl J Med.
LoVecchio, Frank, et al. CDC: May 14, 2024 Drug Overdose Death Rates. Health care cost savings from Australian Poisons Information Centre advice for low risk exposure calls: SNAPSHOT 2. Clinical Toxicology , 58 (7), pp.752-757. “Poison control centers decrease emergency healthcare utilization costs.”
LoVecchio, Frank, et al. CDC: May 14, 2024 Drug Overdose Death Rates. Health care cost savings from Australian Poisons Information Centre advice for low risk exposure calls: SNAPSHOT 2. Clinical Toxicology , 58 (7), pp.752-757. “Poison control centers decrease emergency healthcare utilization costs.”
Common culprits in this situation are tricyclic overdose and cocaine toxicity (remember cocaine not only increases dopamine in central synapses, but is also a local anesthetic (-caine!) The data in the paper by Rangel et al. Lange RA, Cigarroa RG, Flores ED, et al. McCord J, Jneid H, Hollander JE, et al. Vittinghoff, E.
Patients with opiate overdose get naloxone. References American College of Emergency Physicians Clinical Policies Subcommittee on the Adult Psychiatric P, Nazarian DJ, Broder JS, et al. Currier GW, Chou JC, Feifel D, et al. Zaman H, Sampson SJ, Beck AL, et al. Patients with sepsis get antibiotics. Ann Emerg Med.
There have been documented cases of overdose, and of note, there is no known antidote. Sodhi M, Rezaeianzadeh R, Kezouh A, et al. Ahmann AJ, Capehorn M, Charpentier G, et al. Poison centers see nearly 1,500% increase in calls related to injected weight-loss drugs as people accidentally overdose. Bansal AB, Al Khalili Y.
Krantz et al authored a State-of-the-Art Review on Cardiovascular Complications of Opioid Use ( JACC 77(2):205-223, 2021 ) — in which mechanisms from Opioid Overdose that detail arrhythmia production ( up to cardiac arrest ) are elucidated — thereby providing an explanation for the unusual arrhythmias in today's case.
This is pathognomonic of hyperkalemia (I suppose it could be due to a massive overdose of a sodium channel blocking drug, maybe). the associated loss is double, at 200-400 mEq.* [ Sterns RH, et al. She was in shock with thready pulses. A prehospital ECG was recorded: Limb leads: Precordial Leads What is the therapy?
Questions: What are the clinical manifestations of bupropion overdose? How is bupropion overdose treated? How long should a patient be observed after a bupropion overdose? 1 In addition to intentional overdoses, there are multiple case studies of abuse (ingestion, insufflation, injection). hours, SR 3 hours, XL 5 hours.
[display_podcast] Date: August 16th, 2018 Reference: Hohl C et al. display_podcast] Date: August 16th, 2018 Reference: Hohl C et al. Reference: Hohl C et al. Prospective Validation of Clinical Criteria to Identify Emergency Department Patients at High Risk for Adverse Drug Events. AEM Aug 2018. AEM Aug 2018. AEM Aug 2018.
The stepwise approach was guided by vital signs, presence of seizures or focal neurology, presence of trauma (including attempted hanging or cutting), overdoses and substance misuse, level of consciousness, medical complaints, history of alleged sexual assault/rape, and developmental delay. link] Radhakrishnan L, Leeb RT, Bitsko RH, et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content