This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Paramedics provided another 3 sprays of nitro, and 6mg of morphine, which reduced but did not resolve the pain. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. of such ‘high risk Non-STEMI’ patients get angiography within 2 hours.[2] But only 6.4%
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation. The TOMAHAWK Investigators. first appeared on The Skeptics Guide to Emergency Medicine.
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
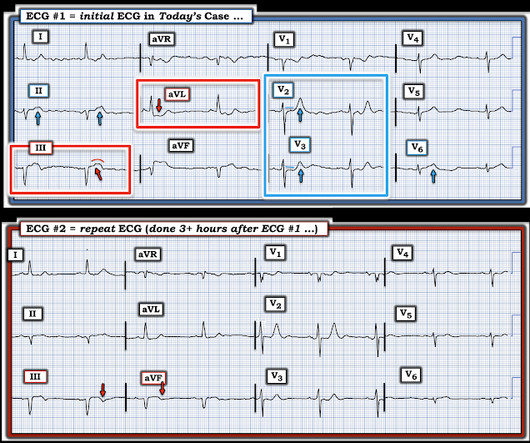
Written by Jesse McLaren Two 70 year olds had acute chest pain with nausea and shortness of breath, and called paramedics. There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. Who needs the cath lab?
Madden, Paramedic. There is mixed overlap of ST-segment elevation (STE), ST-segment depression (STD), Hyperacute T waves (HATW), and deWinter pattern (which the ACC regards as a STEMI-equivalent but is better suited under the blanket of OMI). Let's revisit the deWinter occlusion provided by Paramedic Madden. 2] Costanzo, L.
Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths. The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. Vitals were normal.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith @SmithECGblog I was conducting QA/QI on two very recent cases and was struck by the uniqueness of both. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered.
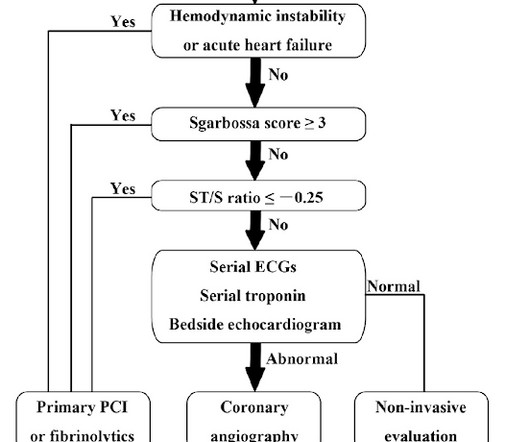
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review and commentary by Dr. Steve Smith [link] @SmithECGblog It is early-summer, approximately 1330 hours, no cloud cover overhead, and 86 degrees with high humidity. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI.
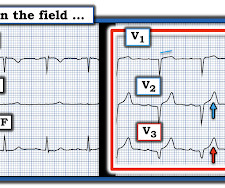
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Expert commentary provided by Dr. Ken Grauer CASE 1 An 82 y/o Male called 911 for sudden onset dizziness while at rest. ASA 324mg was administered while a STEMI activation was simultaneously transmitted to the nearest PCI center. 4] Baranchuk, A, et al.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al.
Clinical Course The paramedic activated a “Code STEMI” alert and transported the patient nearly 50 miles to the closest tertiary medical center. 2 The astute paramedic recognized this possibility and announced a CODE STEMI. Taglieri N, Marzocchi A, Saia F, et al. Kosuge M, Ebina T, Hibi K, et al.
The paramedics found the patient with ROSC and a GCS 7, and an ECG showing LBBB with possible lateral ST elevation. The patient was brought to the ED as a possible Code STEMI and was seen directly by cardiology. On arrival, GCS was 13 and the patient complained of ongoing chest pain.
Here’s the paramedic ECG (digitized by PMcardio). STEMI negative : the EMS automated interpretation read, “STEMI negative. But the latest ACC consensus on the evaluation of chest pain in the ED warns that “STEMI criteria will miss a significant minority of patients with acute coronary occlusion.”[1] What do you think?
Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4. Finally, Transient STEMI should be taken emergently to the cath lab. Normalization of Diagnostic For STEMI Prehospital ECG with Nitroglycerin Therapy. If the initial ECG was diagnostic for STEMI the paramedic called to mobilize the reperfusion team.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review by Dr. Stephen Smith @smithECGblog I was reviewing ECG’s in our LifeNet database and happened upon this one without any knowledge of clinical circumstances. 1] Here is the admitting ED ECG after cancellation of Code STEMI. 1] Driver, B.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith [link] @SmithECGBlog An adult female called 911 for chest discomfort and difficulty breathing. Then, three minutes later… Crews activated STEMI as she deteriorated into PEA arrest. Wolters-Kluwer: Philadelphia, PA. [2]
When the paramedics arrived, they obtained a 12 lead ECG and confirmed the unstable vital signs. There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI).
This was shown to me by a very astute Hennepin paramedic. Although this comes from a Hennepin paramedic, the patient was not brought to Hennepin County Medical Center. It is important for cardiologists to realize that a paramedic may see something they do not. Khan AR, Golwala H, Tripathi A, et al. of this post.
Case submitted by Andrew Grimes, Advanced Care paramedic, with additions from Jesse McLaren and Smith An 84-year-old male with a notable cardiac history (CABG, multiple stents) woke at 0500hrs with pressure in his chest, diaphoresis, and light-headedness. STEMI criteria are only 43% sensitive for OMI.
She was found by paramedics with an oxygen saturation of 64%, but could not tolerate BiPAP during transport due to claustrophobia. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. Truly, the Marquette 12 SL algorithm correctly identifies this STEMI. Management?
The paramedics diagnosis was "Possible Anterolateral STEMI." More proof that a huge STEMI may have normal or near normal initial troponin. Smida T et al. Taken together, these findings suggest an ongoing extensive antero-lateral STEMI. I don't know what the device algorithm interpretation stated.
Here is the written paramedic report available after all the events were over: Patient was seen by witnesses to become unresponsive. A 12-lead was recorded, showing "STEMI," but is unavailable. Moreover, when someone has immediate resuscitation of an arrest witnessed by paramedics, they rarely have a GCS of 3 (deep coma).
This was submitted by a paramedic, Hailey Kennedy A late 50s male called 911 following 2 hours of chest pain that started while working at his desk. The paramedic thought it was LAD OMI, but wasn't certain. The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". Lupu et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content