This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
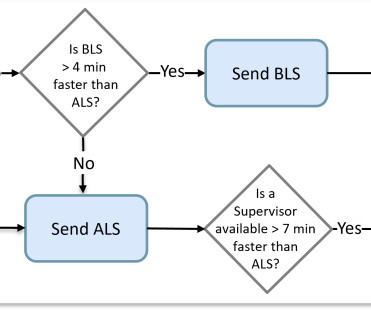
Some computer-aided dispatch (CAD) software did better than others by considering the average travel time of an actual route instead of allowing nearness to be determined by a straight-line distance. If available, the supervisor is added to effectively create an ALS transport ambulance.
Your existing historical CAD records contain the necessary information to build such dynamic views in real-time. The existence of identifiable causes explains the ability to properly forecast the vicinity of calls in addition to their timing.
A 75 yo with h/o CAD, CABG, and HFrEF presented after a syncopal episode. He rehydrated and had no orthostatic symptoms prior to discharge, ambulated well. - There was no prodrome and no associated symptoms such as SOB or CP. The medics recorded an ECG: There is STE in V1-V3 and aVL, with reciprocal ST depression in II, III, aVF.
I hop into the ambulance, and log onto the CAD (Computer Assisted Dispatch) device. The call pops up onto our CAD. I look at the notes on the CAD it read: Crowning. I explain the gravity of the situation to the parents when the second ambulance crew arrives to help out. Me: “Sure, that’s all good with me.”
Of course we get called early in the evening and as we sit inside our ambulance, I hear dispatch announce over the radio… “Code 3 for a testicular bleed…” I remember looking at Jessica thinking… Oh nooo! ” We quickly got back into our ambulance and drove back to the main road.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. CPR was initiated immediately. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation.
I B Ambulance personnel must be trained and equipped to identify STEMI and administer fibrinolysis if necessary. IIa C During hospital stay (after primary PCI) Either stress echo, CMR, SPECT, or PET may be used to assess myocardial ischaemia and viability, including in multivessel CAD.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chest pain. As such, the patient was placed on a heparin drip and transferred by ambulance to a cardiac cath-capable facility. He had an EKG recorded right away.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content