This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
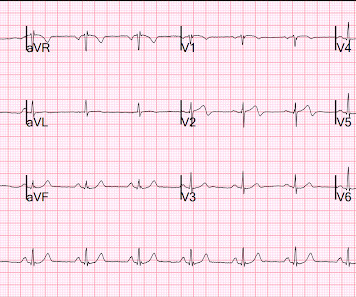
The crew transferred the patient to the ambulance and noticed weak radial pulses (BP unobtainable). Crew notifies the received ED of an incoming post-arrest patient and notes a sinus bradycardia on their monitor, as seen in Figure 2. Pacing was continued in the ED, with identical settings. Several learning points here.
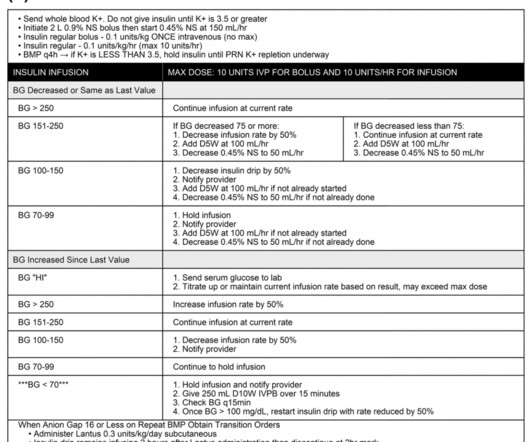
The SQuID protocol (subcutaneous insulin in diabetic ketoacidosis): Impacts on ED operational metrics. The SQuID protocol (subcutaneous insulin in diabetic ketoacidosis): Impacts on ED operational metrics. However, the ICU is full and the patient will likely be boarding in your ED for a bit before coming upstairs.
The patient is re-assessed once secured in the ambulance. Two paramedics are in the rear of the ambulance managing resuscitation (another crew had arrived and provided support with a driver). On ED arrival ROSC is achieved. The crew starts with placing the patient on the monitor, and they notice a heart rate of 60.
The pain makes it difficult for him to ambulate unassisted through his home. About three percent of emergency department (ED) visits are due to skin and soft tissue infections, but data are lacking on the contribution of chronic wounds to this number. Today, he notes worsening swelling and a blister forming near his left ankle.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chest pain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chest pain around 1500 while eating. Patient 2 , EKG 1: What do you think? The patient had none of these conditions.
male with pertinent past medical history including Atrial fibrillation, atrial flutter, cardiomyopathy, Pulmonary Embolism, and hypertension presented to the Emergency Department via ambulance for respiratory distress and tachycardia. Here is the prehospital ECG: First ED ECG What do you think? SVT with aberrancy?
They were randomized to ceftriaxone 2gm intravenous (IV) in the ambulance or usual cares (fluids and supplementary oxygen) until arrive to the ED. A randomized control trial (RCT) done in the prehospital setting enrolled 2,698 patients. For a decision instrument to benefit patients, it needs to have more than a high sensitivity.
Is Use of Warning Lights and Sirens Associated With Increased Risk of Ambulance Crashes? This is Bob’s eleventh visit […] The post SGEM#291: Who’s Gonna Drive you to…the ED – with Lights & Sirens? Is Use of Warning Lights and Sirens Associated With Increased Risk of Ambulance Crashes? Annals of Emergency Medicine.
Approximately 10% of geriatric patients (adults over the age of 65) transported via ambulance will have a mental status altered from baseline, otherwise known as delirium. ED-based protocols have already been created to aid in the treatment of patients with this condition.
1 2 3 4 This article will focus on three lower extremity (LE) nerve blocks commonly used for acute lower extremity pain in the ED. 1 2 3 4 This article will focus on three lower extremity (LE) nerve blocks commonly used for acute lower extremity pain in the ED. Blocks with larger volumes of anesthetic carry higher risk of LAST.
I was about two months into a family practice internship when I went to visit my uncle whose neighbor happened to be an ED resident, Dr. Clarke said. Firsthand Account An ambulance bay at the LA County-USC Hospital in 1978. A cross-country move brought him to Delaware, where he served as the director of a hospital ED in Milford, Del.
Private ambulance companies Most private ambulance companies are always hiring. Positions at ambulance companies tend to be a little more flexible especially for those with other jobs or are in school. It's important to keep in mind that you are not functioning as an EMT when you're an ED Tech/Assistant.
A 50 year old man is brought to your ED by ambulance. He complains of feeling unwell, fever, cough and difficulty breathing. He denies any chest pain or history of previous heart problems. On exami…
Prehospital transdermal glyceryl trinitrate in patients with ultra-acute presumed stroke (RIGHT-2): an ambulance-based, randomized, sham-controlled, blinded, phase 3 trial. Case: Your ambulance responds to a 9-1-1 call for a 75-year-old male experiencing abrupt onset of left sided weakness. The Lancet March 2019. The Lancet March 2019.
In Ontario alone there have been approximately 160 emergency departments (ED) temporarily closed since the beginning of 2022. The dataset also reported increasing admissions, mixed results on length of stay, increasing readmission rates, increasing COPD deaths if transported by ambulance, and expected productivity benefits were not realized.
A 37-year-old G5P4 at 33 weeks presents to the ED after being brought in by ambulance. She had a precipitous delivery while the ambulance was pulling in. We’ll keep it short, while you keep that EM brain sharp. The newborn is doing well, but the mother is complaining of shortness of breath and chest pain.
Methods: This is a retrospective cohort study of agitated patients with an initial Richmond Agitation-Sedation Scale (RASS) score of at least 3, who were sedated and transported by ambulance to Hartford Hospital. There was no difference in endotracheal intubation rates between the two groups (6.1% versus 2.9%, respectively; p = 0.383).
A 12-year-old male is being transported by ambulance after a road traffic accident. A retrospective cohort analysis of the ED portion of the National Hospital Ambulatory Medical Care Survey from 2006 to 2009 in the US revealed that less than one-half of patients undergoing ETI in the ED received sedative drugs while in the ED.
Case: A 62-year-old male with a past medical history of heart failure with reduced ejection fraction presents to your emergency department (ED) via ambulance for palpitations and shortness of breath that started earlier that day. Be critical and evaluate what you believe in.” The remainder of his vital signs are unremarkable.
At one of the hospitals, while my partner finished up the run form in the passenger seat –shed teched the call–I announced I was going back into the ED to the EMS room to see if they had any pizza. I left my glasses in the ambulance. We were on the go. There was a box of pizza there, but only two slices of cheese pizza.
You are working in a rural ED, and an older woman from a local assisted care facility arrives via ambulance in obvious respiratory distress. EMS is able to tell you that she is currently being treated for pneumonia. The patient is on a nonrebreather mask, and vital signs on arrival are BP 110/50 mm Hg, HR 120 bpm, RR 40/min, T 98.6°F
His health care focus included hospital efficiency, physician and patient satisfaction, and emergency department (ED) wait times, as well as a host of nonhealth issues. Today, Dr. Morhaim is donating his time to a recently established Maryland commission focused on ED wait times. His path toward state legislative work was set.
He was unconscious for 8 minutes and slowly awoke in the ambulance, complaining of nausea only. First ED ECG is Wellens' (pain free). This 60 yo male had an apparent tonic clonic seizure. He had no history of seizures. First responders found him to be very tachycardic , confused, perserverating and with no memory of the event.
AEM April 2021 Case: You are sitting minding your own business charting on shift when you become aware of shouting and banging from your ambulance bay. Randomized Double-blind Trial Intramuscular Droperidol, Ziprasidone and Lorazepam for Acute Undifferentiated Agitation in the Emergency Department. Reference: Martel et al.
They concluded: “For patients treated in the ED for opioid overdose, an observation period of one hour is sufficient if they ambulate as usual, have normal vital signs and a Glasgow Coma Scale of 15”. . * Wave 2: Rapid increase in overdose deaths involving heroin starting in 2010.
A 40-something male presented by ambulance with one hour of chest pain that was improving after sublingual nitroglycerine and 325 mg of aspirin, chewed. Here is his initial ED ECG: What do you think? Or had not had a prehospital ECG on the ambulance. Then the ED doc would be dependent on that first ECG.
Ed Bauter We’ve all been there. The AIRWAYS2 trial included four separate ambulance services in the UK, and is the largest data set we have available thus far. What’s the right airway to use? The cardiac arrest that may or may not have a positive outcome depending on what we do as providers. On paper, this is an easy thing to do.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. What do you think?
He advises, however, recurrent syncopal episodes for the past six months, some of which have resulted in ED admission, yet no identifying mechanism could be determined. Steve Smith [link] @SmithECGblog A 72 y/o Male experiences a syncopal episode while seated. It’s reported that he regained consciousness after 30 seconds, approximately.
Patients often seek care in the emergency department (ED) setting when flares of pain affect their ability to ambulate, climb stairs, or even stand up from sitting. In our experience, patients have been able to ambulate comfortably with no motor deficits in approximately 30 minutes. 2,3 Sonoanatomy FIGURE 1. Pain Physician.
Add on the daily frustrations we all face during ED shifts: the challenging consultant, high volumes, time intensive laceration, etc. For me, walking outside the ambulance bay for a few breaths of fresh air or walking to brew a coffee is helpful while I reset. Ask your charge nurse or medical director to walk you through it.
The other night I stood in the trauma bay, listening to rain patter against the automatic doors, awaiting an ambulance. Patient after patient, trauma activation after activation, my trauma surveys became rote and depersonalized by necessity. Or even worse, against their verbal objection. Trauma is unique. 2017;152(9):843.
Ambulance Patient Offload Time (APOT) is a new metric introduced in the 2024 ESO EMS Index that measures the duration from when an ambulance arrives at the hospital to the transfer of patient care to hospital personnel. Ambulances delayed at hospitals mean fewer resources are available for the next emergency call.
Could not ambulate. In ED, repeat potassium level was 2.6 Permanent weakness usually affects the proximal lower extremities, happens in older patients, and develops late. Diagnosis: Can be made in the ED based on history, exam, lab testing. Consult neurology in the ED. Potassium level was 2.0
Grabbing a pristine white table napkin to apply pressure to the wound, Ranulf’s class teacher and expedition leader called the ambulance as chaos descended on the restaurant. All you know, back in ED, is that the ETA is 10 minutes, and there is a single stab wound to the chest. The trauma call goes out.
EMS Environment Ok, we’ve got the patient calmed down and gotten them into the ambulance. If you have restraints in your ambulance, are those restraints appropriately sized for pediatric patients? Protocols Every EMS agency should have protocols for dealing with agitated or violent patients.
One told a frequent patient whose MO was dramatically faking seizures in public places to walk the hell away from the ambulance. Ive never taken him in but Ive seen him, heard him in the ED when others have transported him. Ive seen a number of medics over the years just snap. It doesn’t help getting worked up about it.
Schreyer, MD CMQ FAAE Originally published: Common Sense January/February 2021 The advent and broad availability of ridesharing services, such as Lyft and Uber, are changing the way patients access medical services, and emergency departments (EDs) are taking notice. 5 The cost of transport is also an issue.
Transferring patients from one ED to another hospital is an established part of emergency medicine practice. 1 As fresh challenges of the pandemic and hospital operations changed emergency medicine practice, one of the more challenging areas was the movement of admitted patients out of the first emergency department (ED).
National industry insight reporting from the Australian Industry and Skills Committee suggests that, in 2019 alone, Australia wide, there were over 4,500 enrolments in ambulance and paramedic qualifications1. National Industry Insights: Ambulance and Paramedic. AHPRA's 2019/20 annual report outlines a 14.5% 2019/20 Annual Summary.
His wife contacted the ambulance service after the patient experienced an episode of loss of consciousness. Those who make it to the ED usually have transient occlusions with reperfusion. Written by Magnus Nossen The patient in today's case is a male in his 70s with hypertension and type II diabetes mellitus.
She was brought in by ambulance and received aspirin and nitroglycerin en route. link] Case continued She arrived in the ED and here is the first ED ECG. This originally radiated into her left arm. Over some time and the pain moved into her other arm as well as her jaw. She also had some shortness of breath.
Study idea: We should look at all OMIs who had a chest CT and compare to all patients with Non-OMI pathology who had a contrast chest CT and have radiologists blindly interpret the perfusion of the myocardium The cardiology fellow came down to the ED and said: "What are you worried about? This is diagnostic of posterolateral OMI.
The ambulance report says "BP continued to drop during transport and pt remained cold and clammy." He described it as "10/10" intensity, radiating across his chest from right to left. EMS obtained the following vital signs: pulse 50, respiratory rate 16, blood pressure 96/49. Fortunately, that is exactly what happened.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content