This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chest pain while chopping wood around noon. He wrote most of it and I (Smith) edited.
A 40-something male presented by ambulance with one hour of chest pain that was improving after sublingual nitroglycerine and 325 mg of aspirin, chewed. Here is his initial ED ECG: What do you think? Here it is: Obvious Inferior Posterior STEMI (+) OMI. Or had not had a prehospital ECG on the ambulance.
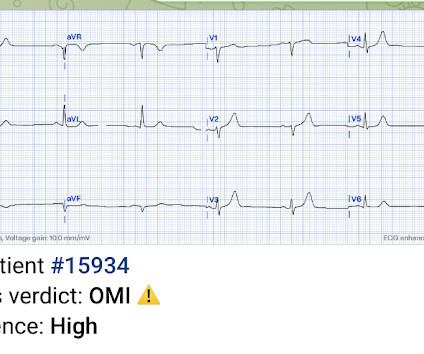
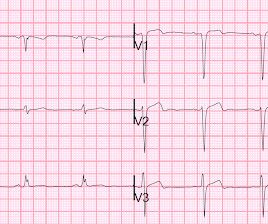
A 61 year-old with chest pain arrived to the ED by ambulance with resolving chest pain. Here is his ED ECG: The computer interpretation was " normal " What do you think? However, when I saw this patient, I knew that he had come by ambulance, so I knew there must be a prehospital ECG recorded somewhere and went to look for it.
She was brought in by ambulance and received aspirin and nitroglycerin en route. link] Case continued She arrived in the ED and here is the first ED ECG. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery.
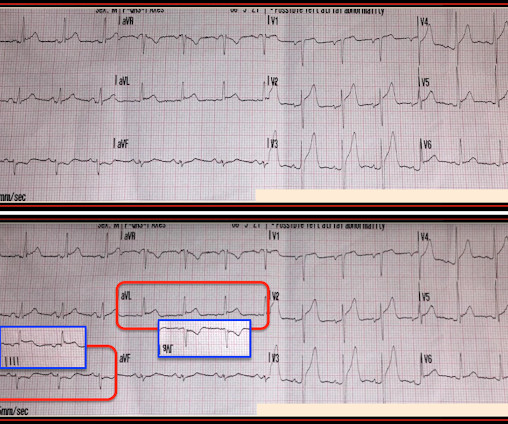
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the Emergency Department via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. What do you think?
The first (and only) ED ECG is here: QTc 386. Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4. Finally, Transient STEMI should be taken emergently to the cath lab. Normalization of Diagnostic For STEMI Prehospital ECG with Nitroglycerin Therapy. Most ST elevation is resolved.
[link] In this paper, in a department in which they state they have only 50 STEMI per year, they looked at only 8 days worth of triage ECGs for a total of 538. They did not find one STEMI on their triage ECGs (no surprise! They only looked at ED diagnosis, not at any angiogram or even at discharge diagnosis. Fair enough.
Ambulated to ambulance for eval. Here it is: The computer reads STEMI What do you think? More from the medic: "LifePak 15 interpretation was STEMI. My response: "I think it is very worrisome for STEMI." It meets STEMI criteria even for a male under age 40, with STE 2.84 No history, meds, or risk factors.
The ambulance report says "BP continued to drop during transport and pt remained cold and clammy." Isn’t it tempting to say there is T-QRS-D in the initial ECG that was done in the ED ( = E CG # 1 in Figure-4 ) ? He described it as "10/10" intensity, radiating across his chest from right to left.
Study idea: We should look at all OMIs who had a chest CT and compare to all patients with Non-OMI pathology who had a contrast chest CT and have radiologists blindly interpret the perfusion of the myocardium The cardiology fellow came down to the ED and said: "What are you worried about? This ST depression?" 2022.08.750 Section 5.2.2,
The medics were worried about STEMI, as it meets STEMI criteria. He rehydrated and had no orthostatic symptoms prior to discharge, ambulated well. - The troponins are NOT consistent with STEMI (OMI), which typically has a troponin I of at least 5 ng/mL. There was no prodrome and no associated symptoms such as SOB or CP.
There is an obvious inferior STEMI, but what else? Besides the obvious inferior STEMI, there is across the precordial leads also, especially in V1. This STE is diagnostic of Right Ventricular STEMI (RV MI). In fact, the STE is widespread, mimicking an anterior STEMI. EKG is pictured below: What do you think?
This is her pre-hospital ECG: This is her first ECG in the ED: What do you think? The nitro she took in the ambulance did not help. She also received an additional nitro in the ED after receiving aspirin and nitro via EMS. Patients like her are the reason we are advocating for a change in the ACS paradigm from STEMI to OMI.
It was a constant ache on the left side of his chest that forced him to stop cycling and call for an ambulance. Figure-1: The initial ED ECG ( = E CG # 1) — with comparison to the patient’s baseline ECG done 4 years earlier ( = E CG # 3). The chest pain started about one hour prior to arrival while bike riding.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. The value of Stat Echo in the ED for confirming clinical and ECG suspicion of acute PE cannot be overstated!
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". He presented to the ED for evaluation chest pain. It was in his central and left chest, radiated to his left arm, and he experienced some cold sweats and nausea prompting him to call 911 and he was brought to ED via ambulance.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content