This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Sepsis) De Winters T waves are the earliest sign of an anterior wall MI but will only be present in ~ 2% of LAD infarcts Patients with Wellens Syndrome on ECG should have a cardiac cath within 24 hours, not necessarily within the first 60 minutes of ED arrival.
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Detailed coronary artery evaluation not performed.
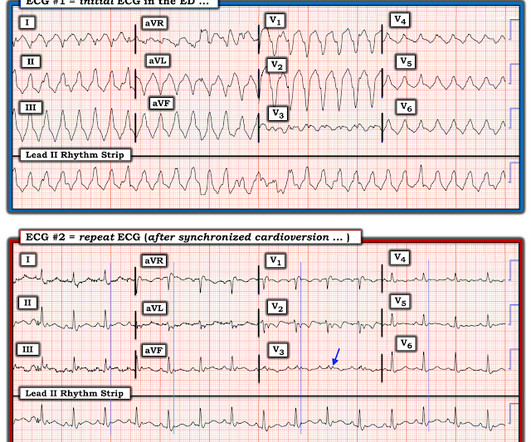
David Didlake EMT-P, RN, ACNP @DidlakeDW An adult male self-presented to the ED with palpitations and the following ECG. Readers of the Smith ECG Blog will probably recognize this a very subtle inferior OMI. The VT vs SVT with Aberrancy debate is beyond the scope of this particular blog post. Here is the ECG after 200J.
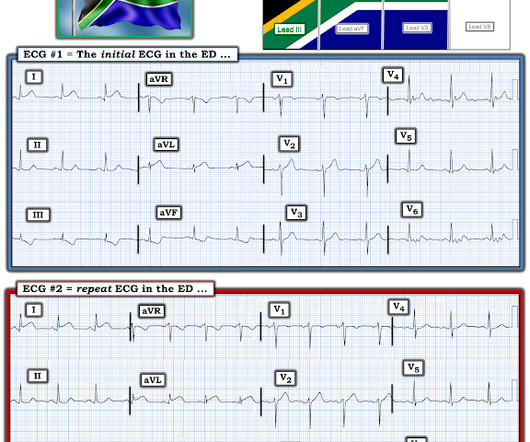
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chest pain. The patient had no chest symptoms until he had been in the ED for many hours and had been undergoing management of his DKA. The patient was under the care of another ED physician. Another ECG was recorded: What do you think?
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Essentially, we are using the troponin assay to find patients with ACO who may be benefited by coronary interventions or risk factor modification. Cardiol Rev.
An undergraduate (not yet in medical school) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly arrived at work and happened to glance down and see this previously recorded ECG on a table in the ED. The young ED tech immediately suspected LAD OMI.
The patient was brought to the ED and had this ECG recorded: What do you think? But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. As we have often emphasized on Dr. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion!
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] It’s judicious, then, to arrange for coronary angiogram.
It was present on arrival at triage but then resolved before bed placement in the ED. This is a demonstration of how Wellens' is transient OMI : First ED ECG is Wellens' (pain free). Also see this incredible case of the use of 12-lead ST Segment monitoring. __ Case Continued The Cath lab was activated 70 minutes after ED arrival.
He has a wonderful #FOAMed blog and podcast called Broomedocs and also work […] The post SGEM#326: The SALSA Study: Hypertonic Saline to Treat Hyponatremia first appeared on The Skeptics Guide to Emergency Medicine. He has a wonderful #FOAMed blog and podcast called Broomedocs and also work with me on the Primary Care RAP team.
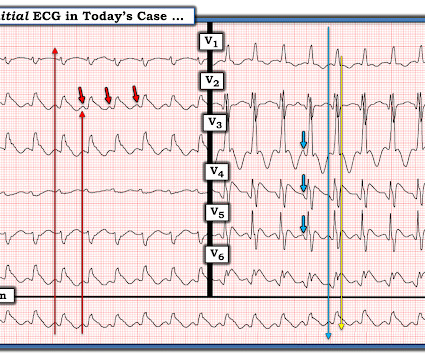
Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ). Figure-1: I've labeled the initial ECG in today's case.
Our data corroborate that immediate management of a patient with a normal automated triage ECG reading is not modified by real-time ED physician ECG interpretation." But troponin is a rear-view mirror which shows damage that has already occurred, and is often within the normal range within only 2 hours of onset of acute coronary occlusion.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. They too have dense white masses consistent with coronary atherosclerosis. Edited by Smith He also sent me this great case.
Coronaries were clean. While statistical likelihood of acute OMI is clearly lower in younger adults — nothing is ruled out by age alone ( as per My Comment in the January 9, 2023 and December 5, 2023 posts in Dr. Smith's ECG Blog ). Sam : "Yes, this case was sent to me. It was a man in his 30s with chest pain. These were all negative.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chest pain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chest pain around 1500 while eating. Patient 2 , EKG 1: What do you think? He went to the cath lab at 0900 the next morning.
Past medical history includes coronary stenting 17 years prior. Initial ED ECG: What do you think? Cardiology was consulted and the patient underwent coronary angiogram which showed diffuse severe three-vessel disease. Coronary angiogram shows diffuse severe three-vessel disease. IV Diltiazem was Contraindicated!
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present."
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. Regular readers of this ECG Blog will be well familiar with many of these points. No ECG was ordered on Day #1.
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). This patient is actively dying from a left main coronary artery OMI and cardiac arrest from VT/VF or PEA is imminent!
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
The patient is an older woman with known coronary disease and an ICD-Pacemaker implanted because of a history of VT ( V entricular T achycardia ). This patient presented to the ED “after a couple of days of chest discomfort”. I have emphasized on many occasions in Dr. Smith's ECG Blog how AFlutter is by far (!)
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL.
But the paramedic and the ED physician in this case did not subscribe to this idea. I have here 38 cases of "Computer Normal" ECGs which were critically abnormal and the vast majority are missed acute coronary occlusions (Missed Acute OMI) and most were recognized by the physician. So this study is worthless and must be ignored.
On arrival to the ED, this ECG was recorded: What do you think? See Discussion in the June 29, 2024 post of Dr. Smith' ECG Blog ). This prompted cath lab activation. There is profound ST depression maximal in V1-V4. Relevance to Today's CASE: As per Dr. Smith — Trying to predict the "culprit" artery in today's case was confusing.
A 40-something with severe diabetes on dialysis and with known coronary disease presented with acute crushing chest pain. Here is his ED ECG: What do you think? As per Dr. Smith — today's patient is a 40-something year old patient with severe diabetes, renal failure and known coronary disease — who presents with “acute crushing CP”.
Here was his initial ED ECG: Formal interpretation by interventional cardiologist: There is "Non-diagnostic" ST Elevation in V2-V4 and aVL. The proof of this is that only 5% of patients enrolled had acute coronary occlusion. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. This study failed to do so.
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. For the same reason, you should not delay coronary angiography because pain resolves with morphine. But pain is a critical signal for urgency in the context of acute coronary syndrome. Mukherjee, D.,
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So the patient had a transient acute coronary occlusion that spontaneously reperfused but is at risk for reocclusion.
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chest pain. It is a known OMI mimic that we have shown on the blog many times. The angiogram showed completely normal coronary arteries.
He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Here is the initial ED ECG. So a dual chamber pacer is placed with one lead through the coronary sinus to the LV.
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." A repeat troponin returned at 0.45 CAD-RADS category 1. --No
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). From there you can link to other great websites (including Dr. Smith's ECG Blog) that provide multiple case studies of both subtle and overt hyperkalemia. Chou's Electrocardiography in Clinical Practice, 6th ed.
showed that among patients with either acute coronary syndrome or acute pulmonary embolism and negative T waves in the precordial leads (V1-V4), that inverted T waves in leads III and V1 were present in only 1% of patients with acute coronary syndrome and 88% of patients with pulmonary embolism. In fact, Kosuge et al.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" Smith and Meyers answer: First , LM occlusion is uncommon in the ED because most of these die before they can get a 12-lead recorded.
Now, it is true that shortly after a non-ACS cardiac arrest, there can be transient diffuse ST depression, but not ST elevation in a coronary distribution, and there should not be a wall motion abnormality. There was faint filling of the distal branches of the RCA by collaterals from the left coronary system.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago.
We have shown many examples of this on this blog. To add to this complexity ( as per My Comment in the August 22, 2020 post in Dr. Smith's ECG Blog ) — the ST-T wave appearance in repolarization variants may be dynamic ! It is clearly missed by the conventional algorithm. No further follow up is available.
Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" On arrival to the ED, while waiting for cath lab team, he obtained another ECG: You can now see the full voltage of the high-voltage QRS, likely with some degree of LVH. Both were awake and alert with normal vital signs.
Because: 1) He has been reading this blog for a long time. He sent the patient to the ED for further evaluation. A chest x-ray in the ED found bilateral pleural effusions. The patient was admitted from the ED and finally had an angiogram the next morning: Angiogram : Image 1: This is the LAO caudal, or spider projection.
He called EMS who brought him to the ED. ED Diagnoses: 1. The basic principles of emergency ECG interpretation in patients who present to an ED with new symptoms include the following: Respect the History. This patient in today's case was a man in his 60s with a known history of coronary disease, including prior stents.
Keep in mind the presenting History ( ie, a 50yo presenting to a rural ED with a 1-hour history of CP radiating to the back and jaw — and an initial ECG labeled as "normal" by the computer interpretation ). As you comtemplate the above issues to address — Take another LOOK at these first 2 ECGs in today's case.
Despite otherwise normal vital signs, she was appropriately triaged to the critical care area of the ED. They are rare and hard to find in normal practice in the ED. For review of a case of RVOT VT — Please see My Comment at the bottom of the page in the February 14, 2022 post in Dr. Smith's ECG Blog.
A man is his late 50’s presents to the ED with 1 hour of post exertional chest pressure associated with diaphoresis and nausea. The ED ECG in the context of the prehospital ECGs was indeed diagnostic of acute coronary occlusion. de Winter's T-waves may occur in any coronary distribution. Both were stented.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content