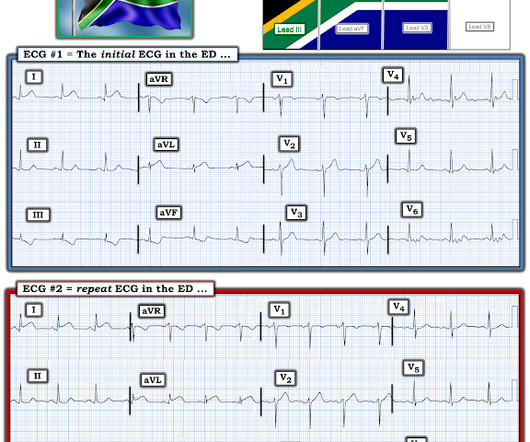
ECG Cases 45 ECG in Weakness and Neurological Symptoms
Emergency Medicine Cases
SEPTEMBER 12, 2023
The post ECG Cases 45 ECG in Weakness and Neurological Symptoms appeared first on Emergency Medicine Cases.
 Blog Coronary OR
Blog Coronary OR 
Emergency Medicine Cases
SEPTEMBER 12, 2023
The post ECG Cases 45 ECG in Weakness and Neurological Symptoms appeared first on Emergency Medicine Cases.

Dr. Smith's ECG Blog
SEPTEMBER 18, 2024
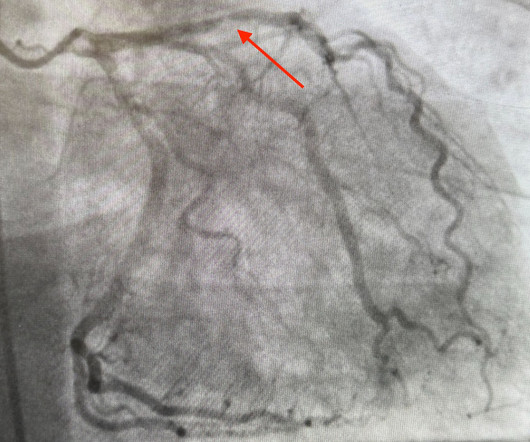
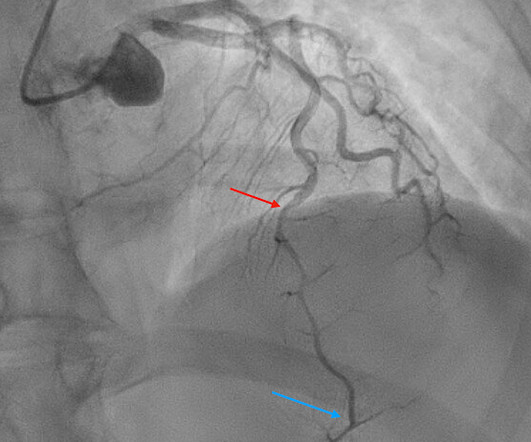
Compensatory enlargement was defined as being present when the total coronary arterial cross-sectional area at the stenotic site was greater than that at the proximal nonstenotic site. Thus, the lumen observed may actually still be the same size as the original, normal lumen. Unfortunately, vascular remodeling is variable and inconsistent.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
Dr. Smith's ECG Blog
JANUARY 2, 2025
Among patients with left bundle branch block, T-wave peak to T-wave end time is prolonged in the presence of acute coronary occlusion. Finally, do a coronary angiogram Possible alternative to pacing is to give a beta-1 agonist to increase heart rate. T-waves are quite tall and possibly peaked (HyperK?), but potassium returned normal.
Emergency Medicine Cases
DECEMBER 16, 2019
In this ECG Cases blog we look at seven patients with potentially ischemic symptoms and subtle ECG changes in the lateral leads. Which had acute coronary occlusion? Introducing the concept of Occlusion MI - a paradigm shift in ECG diagnosis of MI. The post ECG Cases 4: Lateral STEMI or Occlusion MI?

Dr. Smith's ECG Blog
DECEMBER 27, 2023
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. It relies on an 1 mm cut point, which this blog does not favor as an approach to ECG. Guagliumi, G., Iwaoka, R.

Dr. Smith's ECG Blog
NOVEMBER 15, 2023
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. CORONARY ARTERIES: Exam was not directly tailored for coronary artery evaluation, noting recent diagnostic coronary angiogram.

Dr. Smith's ECG Blog
MAY 13, 2024
Dr. Smith and other authors showed the utility of Speckle Tracking Strain Echo in this case report: Diagnosis of acute coronary occlusion in patients with non–STEMI by point-of-care echocardiography with speckle tracking Repeat ECG: Slightly less hyperacute T waves, likely indicating improving flow compared to the first ECG.

Expert insights. Personalized for you.
































Let's personalize your content