This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In this ECG Cases blog we look at 10 patients with potentially ischemic symptoms. Which had a coronary occlusion, and how acute were they? Jesse McLaren explains 'Late STEMI' and how reperfusion strategies should not be based on time of symptom onset. appeared first on Emergency Medicine Cases.
If it looks and feels like a STEMI clinically, get serial ECGs and consult Cardiology immediately. Post Created By: William Caputo MD Post Peer Reviewed By: Anand Swaminathan MD, MPH (Twitter @EMSwami ) The post REBEL Core Cast 104.0 – Subtle ECGs in Acute Coronary Occlusion appeared first on REBEL EM - Emergency Medicine Blog.
10 patients presented with the "STEMI-equivalent" ST elevation in aVR with diffuse ST depression. Which had acute coronary occlusion? Jesse McLaren guides us through the differential diagnosis of ST elevation in aVR with diffuse ST depression in this ECG Cases blog. The post ECG cases 7: ST elevation in aVR, STEMI-equivalent?
In this ECG Cases blog we look at seven patients with potentially ischemic symptoms and subtle ECG changes in the lateral leads. Which had acute coronary occlusion? The post ECG Cases 4: Lateral STEMI or Occlusion MI? Introducing the concept of Occlusion MI - a paradigm shift in ECG diagnosis of MI.
Traditionally, emergency providers looked for signs of ST-segment elevation myocardial infarction (STEMI) to indicate the need for intervention. Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG.
Background: Primary PCI is the recommended reperfusion strategy in patients with STEMI and should be initiated within 2 hours after first medical contact. STREAM-2: Half-Dose Tenecteplase or Primary Percutaneous Coronary Intervention in Older Patients With ST-Segment-Elevation Myocardial Infarction: A Randomized, Open-Label Trial.
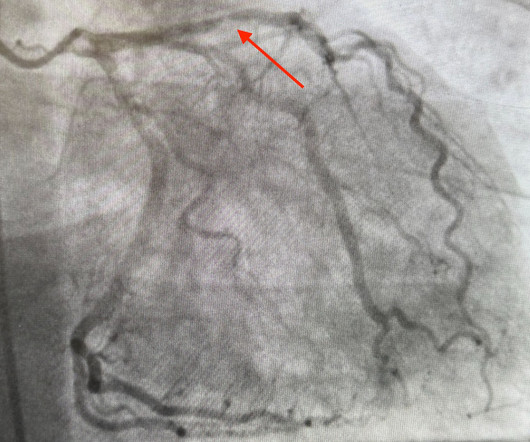
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Compensatory enlargement was defined as being present when the total coronary arterial cross-sectional area at the stenotic site was greater than that at the proximal nonstenotic site. He was started on nitro gtt.
LVH produces secondary repolarization abnormalities that can mimic STEMI. In this ECG Cases blog we look at 6 patients who presented with potentially ischemic symptoms and LVH on their ECG. Which had an acute coronary occlusion?
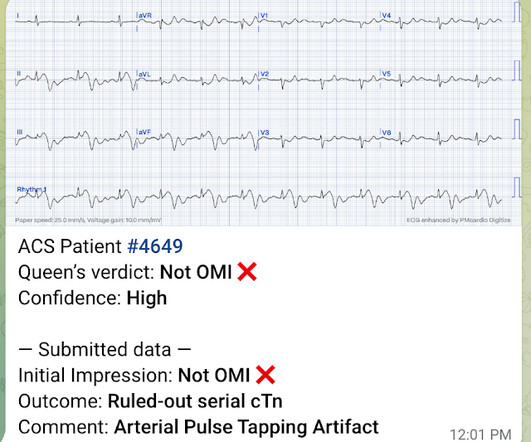
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
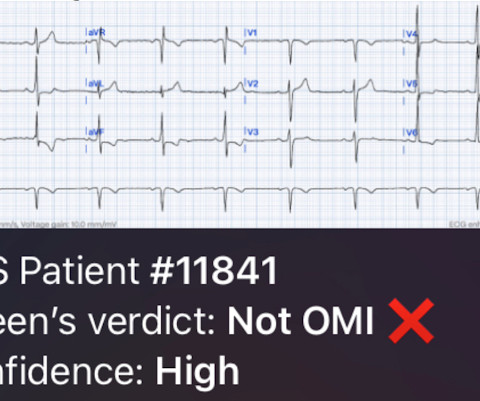
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram.
I came to work one day and one of my partners said, "Hey, Steve, we had a STEMI this afternoon!" That is not a STEMI. More cases can be found on the blog here. They had activated the cath lab and the interventionalist did not notice that it was not a STEMI/OMI. I said, "Cool, can I see the ECG?' He said: "What?
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
But do they represent acute coronary occlusion? But coronaries were normal, and serial high sensitivity troponin was undetectable. Based on ECG changes and echo findings, the patient was diagnosed as coronary vasospasm. Formal echo showed EF 55% with mild inferolateral hypokinesis without any prior for comparison.
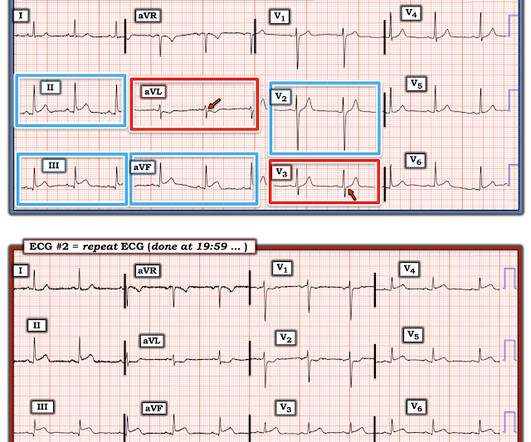
Obvious infero-postero-lateral STEMI(+)OMI, regardless of context Now let’s put them in order: what was the sequence? When the pain recurred the ECG normalized(ECG#2), but this is pseudonormalization : the coronary artery has spontaneously reoccluded, and the T waves are on their way up. What was the outcome and final diagnosis?
But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Cardiac arrest #3: ST depression, Is it STEMI? As we have often emphasized on Dr. Smith's ECG Blog ( See My Comment in the March 1, 2023 post) — DSI does not indicate acute coronary occlusion! And what do you want to do?
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Do NOT give it unless you are committed to the cath lab!! Cath attending is aware. It is a mass delusion.
In this ECG Cases blog we look at 8 patients with potentially ischemic symptoms, to highlight pearls and pitfalls of inferior MI. Can you identify which ones had acute coronary occlusion? The post ECG Cases 3: Can you find the subtle inferior MI? appeared first on Emergency Medicine Cases.
An undergraduate (not yet in medical school) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly arrived at work and happened to glance down and see this previously recorded ECG on a table in the ED. It was recorded at 0530: What do you think?
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. When EMS found her, she was dyspneic and diaphoretic.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. They too have dense white masses consistent with coronary atherosclerosis. Edited by Smith He also sent me this great case.
The proof of this is that only 5% of patients enrolled had acute coronary occlusion. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. This study failed to do so. 5% vs. 58%!!
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later? This caused a type 2 anterior STEMI.
But like many similar studies, the study was small (one year at one centre with no indication of the incidence of acute coronary occlusion), and it used as the gold standard the final cardiologist interpretation of the ECG - not the patient outcome! Despite serial ECGs being "STEMI negative", the cath lab was activated.
This is as clear a STEMI as you can get. Now, it is true that shortly after a non-ACS cardiac arrest, there can be transient diffuse ST depression, but not ST elevation in a coronary distribution, and there should not be a wall motion abnormality. So this is classic inferoposterior STEMI on the ECG but is NOT acute coronary syndrome!
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. Fortunately the patient did not reocclude while awaiting the angiogram.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." For the same reason, you should not delay coronary angiography because pain resolves with morphine. The case continues. Mukherjee, D.,
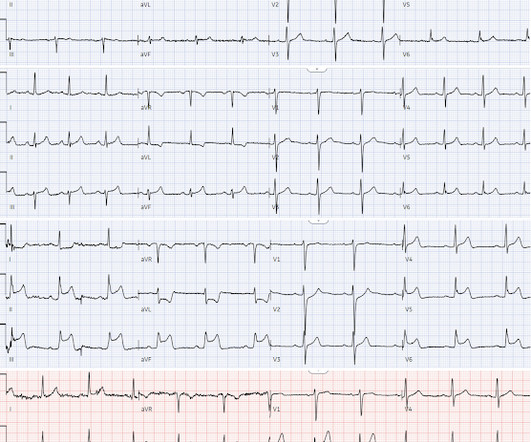
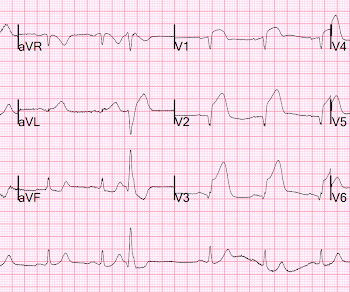
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] STEMI was activated and the patient went to Cath on arrival.
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Learning Points: You cannot trust conventional algorithms even to find STEMI(+) OMI, even when they say "normal ECG." We have shown many examples of this on this blog.
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Meyers, Weingart and Smith published their OMI Manifesto — in which they extensively document the critically important concept that management of acute MI by separation into a “STEMI” vs “non-STEMI” classification is an irreversibly flawed approach.
Posterior leads are unnecessary if anterior leads are diagnostic According to the STEMI paradigm an ECG has to have ST elevation to diagnose acute coronary occlusion, and if there’s no ST elevation on anterior leads you can look for it on posterior leads. Do you need posterior leads? If so, how will they change management?
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Additionally, his cardiac telemetry monitor showed runs of accelerated idioventricular rhythm, a benign arrhythmia often associated with coronary reperfusion.
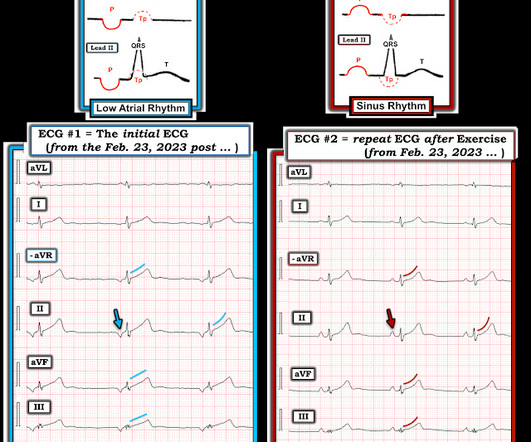
In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. In other words, the inferior "ST elevation" is due to the abnormal rhythm, and does not signify OMI or STEMI in any way. It is a known OMI mimic that we have shown on the blog many times.
According to this data a triage ECG labeled ‘normal’ rules out the possibility of acute coronary occlusion. This is obviously unreliable data, as Dr. Smith’s Blog has published 51 cases of OMI with ECGs labeled ‘normal’ , 35 of which were identified by the Queen of Hearts – with 10 examples here.
Methods and Results Patients with confirmed ST elevation myocardial infarction (STEMI) treated by emergency medical services were included in this retrospective cohort analysis of the AVOID study. Greater severity of chest pain is presumed to be associated with a stronger likelihood of a true positive STEMI diagnosis. years old ± 13.7
? OMI Pocket Guide The OMI Pocket Guide ( [link] ) is a user-friendly online resource designed to help healthcare professionals learn how to recognize subtle signs of acute coronary occlusion on the ECG which represent occlusion myocardial infarctions (OMI). Smith and Meyers ( that are well known to readers of this Blog ).
At the hospital a 12-lead ECG is recorded within 10 minutes and read by the attending physician, who activates the “Code STEMI” protocol. Is this a STEMI? So technically it is a STEMI equivalent. The STEMI guidelines require 2 mm of ST-segment elevation in leads V2 and V3 for men (1.5 The answer is yes!
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). No ECG was ordered on Day #1.
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. ng/mL and 0.10
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content