This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
You continue with compressions and defibrillations and your partner places an advanced airway. The patient is a 54-year-old man who collapsed in front of his family after complaining of chest pain for several hours. On your arrival, first responders from the fire department are performing high-quality basic cardiac life support.
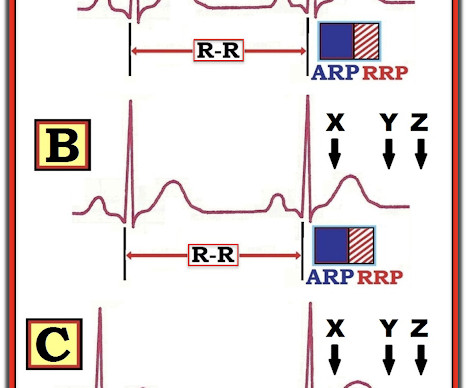
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. IF the initial ECG following successful defibrillation shows evidence of acute OMI — such patients have much to gain from immediate cath with PCI. As per Dr. Smith — the intuitive answer should be obvious.
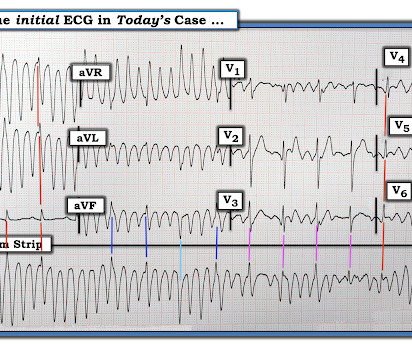
15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. Meyers and Smith in the October 15, 2022 post of Dr. Smith's ECG Blog ). Written by Pendell Meyers A man in his 50s was found by his family in cardiac arrest of unknown duration. Further information is not available.
Josh Kimbrell, NRP @joshkimbre Judah Kreinbrook, EMT-P @JMedic2JDoc This is the first installment of a blog series showing how transcutaneous pacing (TCP) can be difficult, and how you can improve your skills. TCP In Transit: A case reviewing transcutaneous pacing, false electrical capture, and re-arrest.
In this CritCases blog Michael Misch takes us through a case of accidental hypothermia and cardiac arrest, reviewing the controversies in management as well as the guidelines for rewarming, the role of ECMO and the alterations to ACLS cardiac arrest medications, CPR and defibrillations.
Because she has cardiomyopathy and ventricular dysrhythmias, the pacer included an Implanted Cardioverter-Defibrillator (ICD) Echo 6 days later after CRT: Normal estimated left ventricular ejection fraction. The septum is punctured with the active fixation screw of the lead - so essentially you bore the septum with the screw helix."
Background Information: Double external defibrillation (DED) is an intervention often used to treat refractory ventricular fibrillation (RVF). This procedure involves applying another set of pads attached to a second defibrillator to a patient and shocking them in hopes of terminating the rhythm. N Engl J Med.
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR. This patient was witnessed by bystanders to collapse. They started CPR. EMS arrived and found him in Ventricular Fibrillation (VF).
He required multiple defibrillations within a period of a few hours. This time, the arrhythmia did not spontaneously terminate — but rather degenerated to VFib, requiring defibrillation. Some episodes of PMVT would terminate spontaneously — but on many occasions, the PMVT degenerated to VFib, requiring defibrillation.
Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. Much depends on the post resuscitation ECG and its evolution shortly after defibrillation. Does this patient have ACS? Should he necessarily go to the cath lab?
He underwent further standard resuscitation EXCEPT that we applied the Inspiratory Threshold Device ( ResQPod ) AND applied Dual Sequential Defibrillation (this simply means we applied 2 sets of pads, had 2 defib machines, and defibrillated with both with only a fraction of one second separating each defibrillation.
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. There was no bystander CPR.
She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal life support). After good ECMO flow was established, she was successfully defibrillated. Here is a case of ECMO defibrillation with near shark fin that was due to proximal LAD occlusion. The K was normal.
We also gave insulin and furosemide (which take much longer to have their effect) After episodes of asystole and VF with defibrillation, she obtained ROSC and this 12-lead was recorded: The monitor around this time was NOT showing a very wide complex What do you think? How would you treat?
VF was refractory to amiodarone, lidocaine, double-sequential defibrillation, esmolol, etc. Then the patient would have been taken to the critical care area with a defibrillator at his side while waiting for the cath lab to be ready. Resuscitative attempts were initiated quickly. Eventually asystole, and the patient died.
Known cardiac defibrillator. appeared first on REBEL EM - Emergency Medicine Blog. Indication for emergency invasive coronary angiography or had coronary angiography within 1 hour of arrival. Known obstructive coronary artery disease or known coronary stent. Pre-existing DNR order. Severe renal dysfunction.
She was successfully revived after several rounds of ACLS including defibrillation and amiodarone. In our hope of increasing appreciation of the clinical insights that this fascinating phenomenon may provide — we highlight its occurrence in our blog posts. On arrival to the ED the patient was intubated with normal vital signs.
But artifact is "alive and well" — and learning to recognize it will amaze many of your colleagues ( and may serve to avoid an unnecessary defibrillation or two ). Like most clinicians — I learned about artifact "the hard way" = by seeing clinical cases that initially fooled me.
She was successfully defibrillated and taken back to the ED. They also sued both EMTs for allegedly not starting chest compressions and defibrillating quickly enough. The physician documented that she was “improved” and the patient was discharged. The following morning, the patient collapsed in the kitchen in front of her family.
This episode self terminated before defibrillation was possible. For review of how Systematic 12-Lead ECG Interpretation not only increases accuracy, but also speeds you up — Please check out ECG Podcast #1 , wit h outline and link to my talk on this subject in the July 24, 2024 post in Dr. Smith's ECG Blog.
Today's case reminds us of the intuitive logic that if a patient has a shockable arrest ( ie, VFib ) — and following successful defibrillation shows evidence of acute OMI ( even if STEMI criteria are not necessarily fulfilled ) — that such patients have much to gain from immediate cath with PCI. (
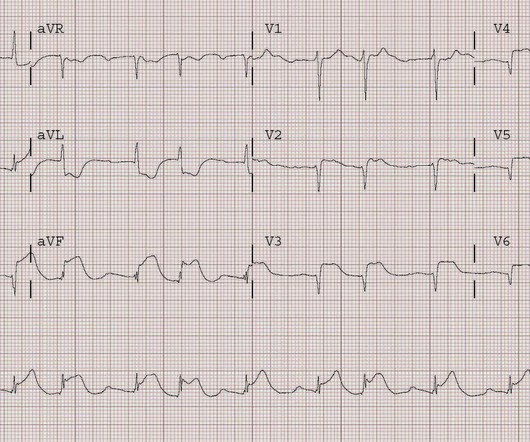
Adapted from Dr. Smith’s EKG Blog. Defibrillator pads are placed and you give 2 g IV magnesium over ten minutes. It is recommended to use an unsynchronized setting as the defibrillator may not be able to track the R-wave in the polymorphic waveform. An ECG is performed and is shown below: Figure 1. She denies chest pain.
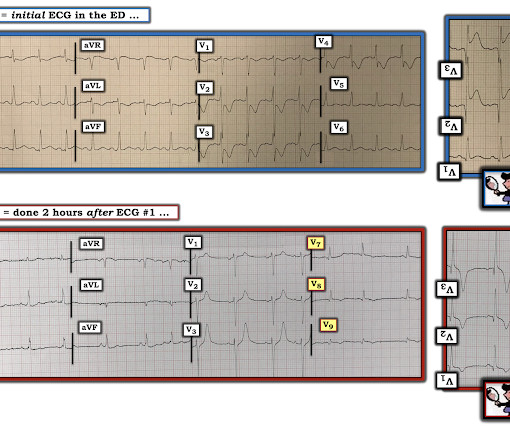
Two hours later , the patient returned to this same urgent care facility with worsening chest pain, and this ECG was performed: While getting another ECG, the patient suffered cardiac arrest: After multiple defibrillations, ROSC was achieved with ongoing "STEMI". The LCX was noted to be "subtotally stenosed" at the time of cath.
The arrhythmia spontaneously converted before defibrillation was achieved. Just prior to arrival he fell out of consciousness with the below ECG on the monitor. ECG #3 The above ECG shows a polymorphic VT at a rate of about 180 BPM.
She spontaneously converted (Defibrillation was not performed). Most such rhythms in the setting of ischemia are VF and will not convert without defibrillation. The patient was given chest compressions while waiting for the cardiac arrest team to arrive. After about 90 seconds of chest compressions she awoke.
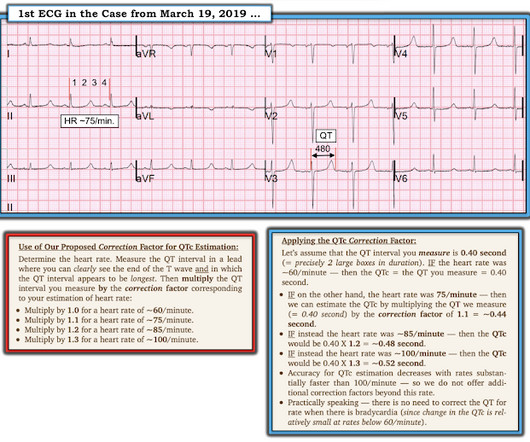
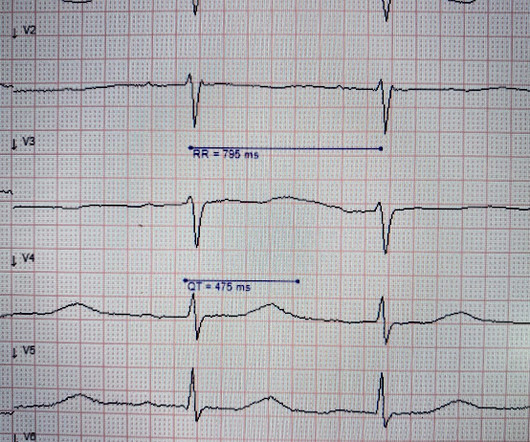
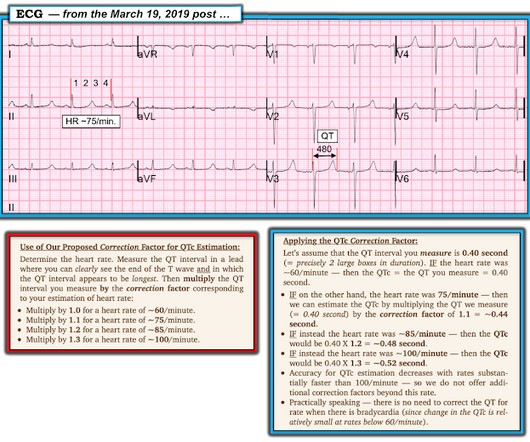
Figure-2: A rapid method for estimating the QTc ( Figure from My Comment in the March 19, 2019 post in Dr. Smith's ECG Blog ). == Clinical Implications of a Short QTc: The differential diagnosis for today's tracing, with its short QTc ~360 msec. Treatment is by ICD ( implantable cardioverter defibrillator ).
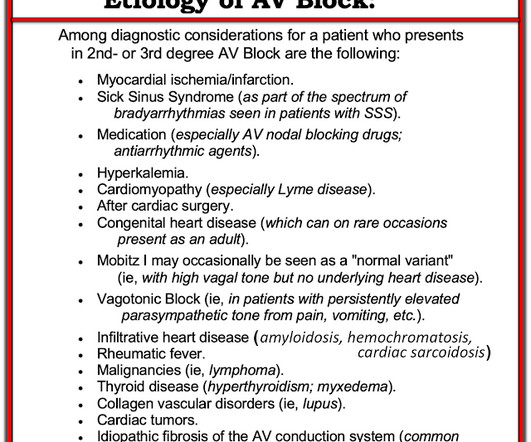
She was given CRT-D (Cardiac Resynchronization Therapy-Defibrillator). Learning points: == MY Comment , by K EN G RAUER, MD ( 1/15 /2024 ): == Today's case by Dr. Nossen differs from other cases of AV block we have published over the years in Dr. Smith's ECG Blog — in that the cause of AV block turned out to be CS ( C ardiac S arcoidosis ).
After resuscitation and defibrillation , there were no more episodes of TdP. Below is the patient’s 12 lead ECG following defibrillation. Of note — the QT interval of beat #5 ( blue line ) is markedly prolonged compared to the QT interval in the beginning of the tracing ( red line ). What does this ECG tell you?
After amiodarone and several defibrillations and about 20 minutes after initial arrest, stable ROSC was achieved. How did the PM Cardio Queen of Hearts perform: Not OMI with low confidence. ECG#3 Resuscitation efforts were ongoing. ROSC was achieved shortly before new episodes of ventricular tachycardia.
As worrisome as the initial recording in leads I and II look — a glance at lead III should immediately reassure us that defibrillation is not needed! I thoroughly reviewed this concept ( as well as other helpful clues to the presence of artifact ) in My Comment — at the bottom of the page in the August 26, 2022 post in Dr. Smith’s ECG Blog.
Background: There are only two interventions that have been proven in the medical literature to improved outcomes in cardiac arrest: high-quality CPR and early defibrillation. There is No Association with Improved Outcomes for Head Up CPR: Why We Must Read Past the Abstract appeared first on REBEL EM - Emergency Medicine Blog.
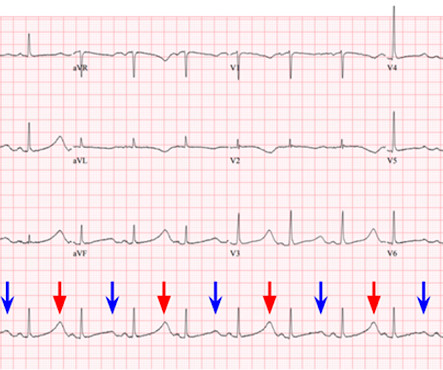
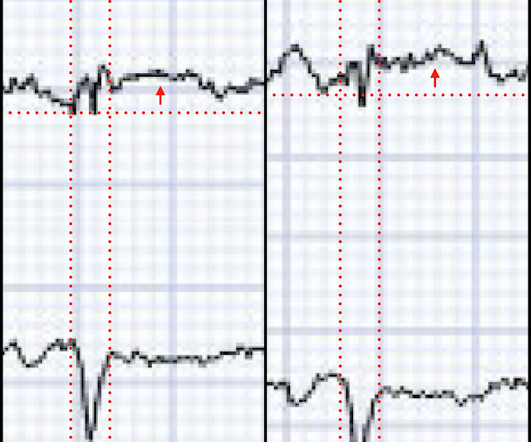
EMS report was that the patient had unknown down time with unwitnessed arrest, found initially in VFib arrest, defibrillated x1 followed by PEA arrest alternating with asystolic arrest during transport. Upon closer inspection, the defibrillator's monitor had assigned a spike for every large T wave as well as every QRS complex.
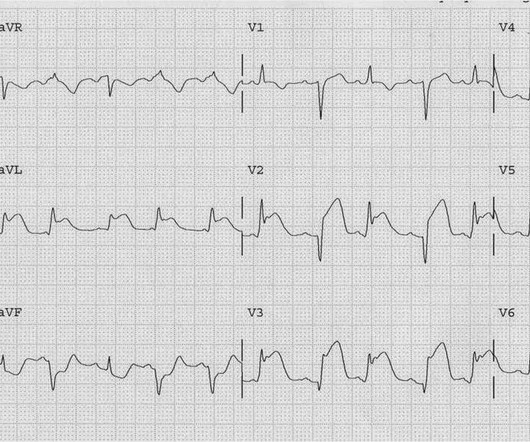
ECG 2 Especially in the context of the first ECG, readers of this blog will readily appreciate the ST elevations and hyperacute T waves in II, III, aVF, V6, and to a lesser extent V5. As discussed on this blog many times before, proportionality is key to the diagnosis of OMI by ECG. [link] I also texted the ECG to Dr. Smith.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She was immediately intubated during continued compressions, then underwent a 9th defibrillation, which resulted in an organized rhythm at 42 minutes after initial arrest. References : 1.
She was defibrillated successfully from ventricular fibrillation and developed a perfusing rhythm. A 56 yo f with h/o HTN and hypercholesterolemia called EMS from home after onset of L chest pain radiating to the left arm. Before EMS arrived, she had "seizure activity" and became unresponsive. She was intubated.
The patient had 2 ventricular fibrillation arrests during transport, but was immediately defibrillated both times, and was awake in the ED, when the following ECG was recorded: The ST elevation has mostly resolved on this ECG, and were it not for the arrest and the prehospital ECG, this would not be a slam dunk diagnosis.
He was resuscitated with chest compressions and defibrillation and 1 mg of epinephrine. This young male had ventricular fibrillation during a triathlon. On his bib it stated that he had a congenital heart disorder. He arrived in the emergency department hemodynamically stable. His initial ECG is shown here.
He was found in ventricular fibrillation and defibrillated, then brought to a local ED which does not have a cath lab. This blog is full of cases in which OMI that did not meet STEMI millimeter criteria were dismissed. Smith’s ECG Blog ). Here is the initial ED ECG: This is pretty obviously and inferior posterior OMI, right?
This blog post explores how your donations can significantly impact first responders, enhancing their capabilities and ensuring they can continue to perform their duties effectively and safely. For instance, donations can fund thermal imaging cameras that allow firefighters to see through smoke and locate individuals in burning buildings.
But after reading this blog, you all know that most OMI do NOT meet STEMI criteria. Defibrillated out of v fib in the cath lab. I thank you for constantly updating your blog and allowing free open access education on EKG interpretation. mm in men over age 40. So there is definitely no STEMI, and the STE is normal.
This is another case written by Pendell Meyers (who is helping to edit the blog and has many great recent posts) Case A 45 year old man was driving to work when he experienced acute onset sharp left sided chest pain with paresthesias of the left arm. He received aspirin en route via EMS, and no EMS ECGs are available.
He was defibrillated. The formula results in 23.43, just above the 23.4 The patient was diagnosed with esophageal reflux and was being discharged by the nurse when he had a cardiac arrest. Here is his post resuscitation ECG: Now the diagnosis is obvious. Anterolateral STEMI.
But because Dr. Mastoras recognized the hyperacute T waves, the patient was immediately seen, the polymorphic VT was immediately defibrillated, and the patient was rapidly diagnosed and treated. For more on this topic — See discussion in the October 24, 2019 and July 31, 2018 posts in Dr. Smith's ECG Blog ).
The patient was put on Extracorporeal Life Support in the ED 3 hours after initial resuscitation, the core temp was 30° C and the patient was defibrillated with a single attempt. On arrival, CPR was continued and core temperature was measured at 18° C (64.4° A 12-lead ECG was recorded: There is sinus rhythm with RBBB and right axis deviation.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content