This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Josh Kimbrell, NRP @joshkimbre Judah Kreinbrook, EMT-P @JMedic2JDoc This is the first installment of a blog series showing how transcutaneous pacing (TCP) can be difficult, and how you can improve your skills. On ED arrival ROSC is achieved. They are unable to feel a pulse and resume CPR.
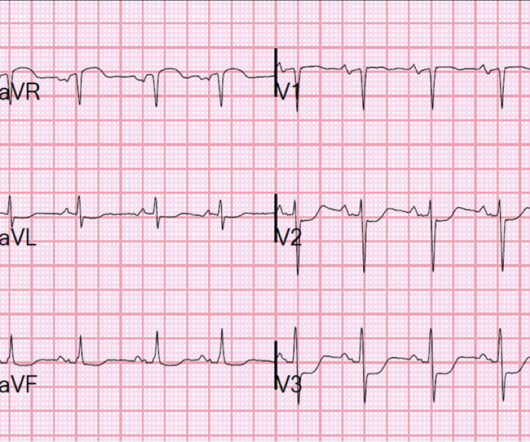
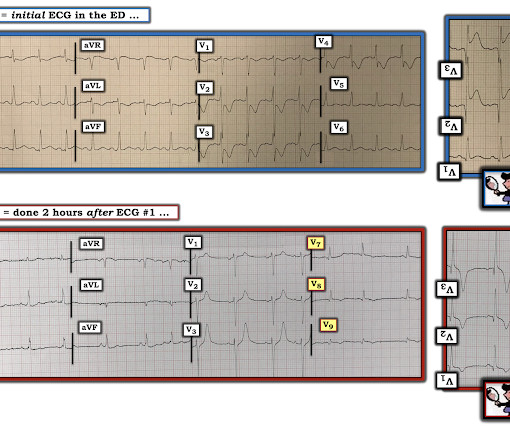
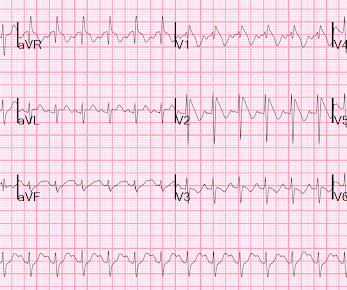
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. Here was his initial ED ECG: Formal interpretation by interventional cardiologist: There is "Non-diagnostic" ST Elevation in V2-V4 and aVL. As per Dr. Smith — the intuitive answer should be obvious.
15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. Meyers and Smith in the October 15, 2022 post of Dr. Smith's ECG Blog ). His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. Further information is not available.
He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. The patient was brought to the ED and had this ECG recorded: What do you think? See these related cases: Cardiac arrest, defibrillated, diffuse ST depression and ST Elevation in aVR. After 1 mg of epinephrine they achieved ROSC.
He was defibrillated, but they also noticed that he was being internally defibrillated and then found that he had an implantable ICD. He was unidentified and there were no records available After 7 shocks, he was successfully defibrillated and brought to the ED. Here is the initial ED ECG. What do you think?
Here was his initial ED ECG: There is atrial fibrillation with a rapid ventricular response. Again, it is common to have an ECG that shows apparent subendocardial ischemia after resuscitation from cardiac arrest, after defibrillation, and after cardioversion. A middle-aged male had a V Fib arrest. He had a history of CAD with CABG.
A 40-something with persistent Ventricular Fibrillation presented after attempted prehospital resuscitation A 40-something with no previous cardiac history presented to the ED in persistent Ventricular Fibrillation after attempted prehospital resuscitation. Finally, head-up CPR (which was not used here), makes for better resuscitation.
She was unable to be defibrillated but was cannulated and placed on ECMO in our Emergency Department (ECLS - extracorporeal life support). After good ECMO flow was established, she was successfully defibrillated. Here is a case of ECMO defibrillation with near shark fin that was due to proximal LAD occlusion. The K was normal.
VF was refractory to amiodarone, lidocaine, double-sequential defibrillation, esmolol, etc. Then the patient would have been taken to the critical care area with a defibrillator at his side while waiting for the cath lab to be ready. Resuscitative attempts were initiated quickly. Eventually asystole, and the patient died.
Click here to sign up for Queen of Hearts Access Case A 58-year-old woman presented to the ED with burning chest pain that started 2-3 hours earlier while sitting on a porch swing. Here is her ED EKG: What do you think? She was successfully defibrillated and taken back to the ED. But which artery? The family sued.
She was successfully revived after several rounds of ACLS including defibrillation and amiodarone. On arrival to the ED the patient was intubated with normal vital signs. In our hope of increasing appreciation of the clinical insights that this fascinating phenomenon may provide — we highlight its occurrence in our blog posts.
Adapted from Dr. Smith’s EKG Blog. Defibrillator pads are placed and you give 2 g IV magnesium over ten minutes. It is recommended to use an unsynchronized setting as the defibrillator may not be able to track the R-wave in the polymorphic waveform. A simplified standard protocol for ED management is below 3.
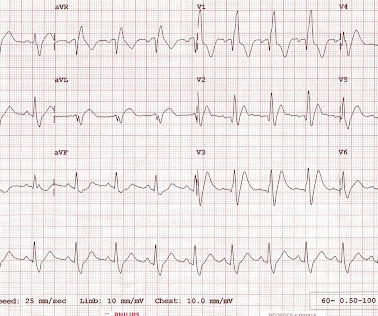
On arrival to the ED, this ECG was recorded: What do you think? See Discussion in the June 29, 2024 post of Dr. Smith' ECG Blog ). This prompted cath lab activation. There is profound ST depression maximal in V1-V4.
In this medical system, the EMS provider can then be routed to the ED or to a type of urgent care facility that is open 24 hrs/day and staffed by a primary care provider. In this case, the EMS provider was routed to the urgent care facility. The LCX was noted to be "subtotally stenosed" at the time of cath.
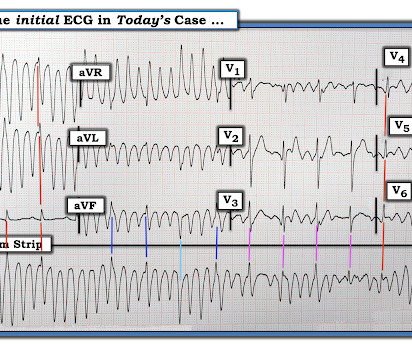
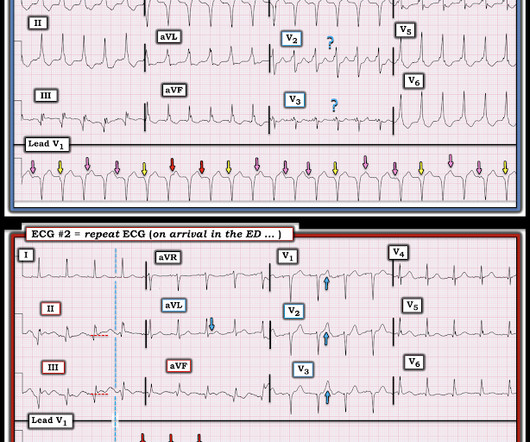
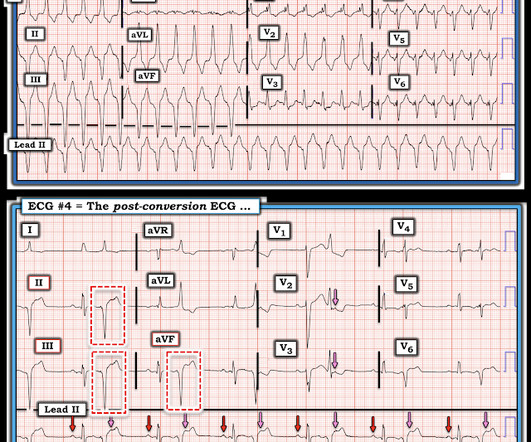
The arrhythmia spontaneously converted before defibrillation was achieved. Those who make it to the ED usually have transient occlusions with reperfusion. Just prior to arrival he fell out of consciousness with the below ECG on the monitor. ECG #3 The above ECG shows a polymorphic VT at a rate of about 180 BPM.
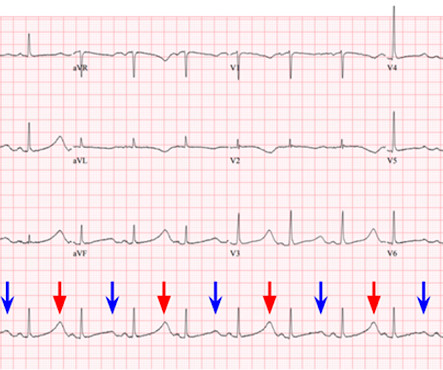
EMS report was that the patient had unknown down time with unwitnessed arrest, found initially in VFib arrest, defibrillated x1 followed by PEA arrest alternating with asystolic arrest during transport. Upon closer inspection, the defibrillator's monitor had assigned a spike for every large T wave as well as every QRS complex.
Submitted by Dr. Arjun J V in India, An elderly patient presented to the ED with multiple complaints. As worrisome as the initial recording in leads I and II look — a glance at lead III should immediately reassure us that defibrillation is not needed! An ECG was recorded in triage: What do you think?
The patient had 2 ventricular fibrillation arrests during transport, but was immediately defibrillated both times, and was awake in the ED, when the following ECG was recorded: The ST elevation has mostly resolved on this ECG, and were it not for the arrest and the prehospital ECG, this would not be a slam dunk diagnosis.
This is another case written by Pendell Meyers (who is helping to edit the blog and has many great recent posts) Case A 45 year old man was driving to work when he experienced acute onset sharp left sided chest pain with paresthesias of the left arm. This was brought to the ED physician who interpreted this as unchanged from initial ECG.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. She arrived in the ED 37 minutes after 911 was called, with continuing CPR. at the time of the ECG.
He was found in ventricular fibrillation and defibrillated, then brought to a local ED which does not have a cath lab. Here is the initial ED ECG: This is pretty obviously and inferior posterior OMI, right? This blog is full of cases in which OMI that did not meet STEMI millimeter criteria were dismissed.
But after reading this blog, you all know that most OMI do NOT meet STEMI criteria. Defibrillated out of v fib in the cath lab. I thank you for constantly updating your blog and allowing free open access education on EKG interpretation. Figure-1: The initial ECG done in the ED ( See text ). mm in men over age 40.
ECG 2 Especially in the context of the first ECG, readers of this blog will readily appreciate the ST elevations and hyperacute T waves in II, III, aVF, V6, and to a lesser extent V5. As discussed on this blog many times before, proportionality is key to the diagnosis of OMI by ECG. [link] I also texted the ECG to Dr. Smith.
Submitted by Dr. George Mastoras (Twitter @georgemastoras), written by Jesse McLaren It’s a busy day in the ED when you’re sent another ECG to sign off from a patient at triage. For more on this topic — See discussion in the October 24, 2019 and July 31, 2018 posts in Dr. Smith's ECG Blog ).
The patient was put on Extracorporeal Life Support in the ED 3 hours after initial resuscitation, the core temp was 30° C and the patient was defibrillated with a single attempt. This Transesophageal ED Echo was recorded: Cardiac POCUS.mov from Stephen Smith on Vimeo. In all leads, there is a 2nd wave after the initial QRS.
When the ICD was finally interrogated, the syncopal events and shocks correlated with two VF events that were defibrillated successfully. That this might happen should not be surprising — since the patient's chest pain was already ongoing for 3 hours prior to arrival in the ED.
She was never defibrillated. I was texted this ECG in real time, but it turns out to actually be the 2nd one recorded in the ED. ECG #4 — This is the 3rd ECG that was done in this case ( obtained ~1 hour after arrival in the ED ). As was seen in this case — defibrillation and/or overdrive pacing may be needed.
She was never seen to be in ventricular fibrillation and was never defibrillated. She was hypotensive in the ED and her bedside echo showed a normal RV and LV. Two prehospital 12-lead ECGs looked similar to this ED ECG: This shows diffuse ST depression (I, II, III, aVL, aVF, V3-V6) with reciprocal ST elevation in lead aVR.
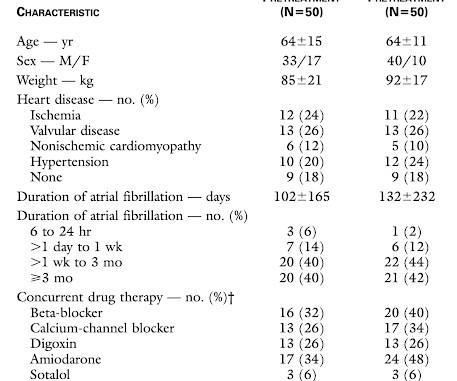
We examined the effect of ibutilide, a class III antiarrhythmic agent, on the energy requirement for atrial defibrillation and assessed the value of this agent in facilitating cardioversion in patients with atrial fibrillation that is resistant to conventional transthoracic cardioversion. Methods. . =
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation. CPR was initiated immediately.
If the patient only had these two ECGs recorded, it would have missed the transient time between them which were STEMI positive, and the patient would then have arrived at the ED as “serial ECGs STEMI negative." There was 100% proximal LAD occlusion, EF was 55% with severe hypokinesis to mid-distal septum and apex.
-- Comment by K EN G RAUER, MD ( 1/30/2019 ): -- Superb presentation and discussion by Dr. Alexandra Schick ( with edits by Dr. Smith ) of an elderly woman who was seen in the ED for altered mental status, hyperthermia, and the initial ECG shown above.
Only 5-18% of ED patients with chest pain have a myocardial infarction of any kind. Cardioversion/defibrillation. Could this be a coincidence that the patient was experiencing chest pain and upon ECG capture the atypical brugada pattern was found? Answer : History is insensitive and nonspecific. It helps a little bit. Hypothermia.
She was defibrillated and resuscitated. To Emphasize: The reason definitive diagnosis is important in today's case — is that the senior ED physician interpreted ECG #1 as "nothing too exciting". Upon arrival to the emergency department, a senior emergency physician looked at the ECG and said "Nothing too exciting."
They transported to the ED. The history, obtained subsequently, is interesting: The patient had been seen at an outside ED 2 days prior and the K was 2.5 Hospital admission had been recommended, but she left that ED against medical advice. What does a heart look like on ultrasound when the EKG looks like that?
Here is his ED ECG: There is obvious infero-posterior STEMI. At cath, he immediately had incessant Torsades de Pointes requiring defibrillation 7 times and requiring placement of a transvenous pacer for overdrive pacing at a rate of 80. Medics stated that he had not been taking his clopidogrel for 2 weeks. He appeared to be in shock.
Features of Short QT Syndrome: From My Comment at the bottom of the page in the September 2, 2019 post of Dr. Smith’s ECG Blog: SQTS is an inherited cardiac channelopathy determined by the presence of symptoms ( syncope, cardiac arrest ) — positive family history — and the ECG finding of an abnormally short QTc interval.
--If she has fever, she should aggressively take acetaminophen and/or ibuprofen and, if not improving, will need to go to ED for further evaluation. --If If there are any syncopal or presyncopal events, she should be evaluated immediately in the ED. --All All 1st degree relatives should have 1 time EGG. 8, 2019 ) — ( Jan.
Soon after the witnessed occlusion, the patient suffered ventricular fibrillation arrest, from which he was immediately resuscitated with 1 defibrillation. Patients with complete left main occlusion usually die before arrival in the ED. This ECG is taken from the July 25, 2024 post in Dr. Smith's ECG Blog.
Defibrillation was performed, and ROSC was achieved. This patient is a man in his 60s who presented to the ED with new CP. Figure-2: Handy link to LVH Criteria ( conveniently placed in the menu at the top of every page in Dr. Smith's ECG Blog ). He was sent back to the waiting room, where he suffered a VF arrest.
The submitter started the patient on amiodarone and arranged implantation of a defibrillator. == MY Comment , by K EN G RAUER, MD ( 12/27 /2024 ): == Superb discussion by Dr. Frick in today's case, that highlights a series of important points regarding the ECG recognition of stable VT ( V entricular T achycardia ).
This is what the providers in the ED understood on patient arrival: Patient called 911 for syncope, then had witnessed PEA arrest after medics arrived. She was brought to the ED in a deep coma with GCS of 3, with vital signs, and an ECG was recorded: What do you think? Not a shockable rhythm. including epinephrine, and there was ROSC.
Throughout this process, the patient had repeated VF and was defibrillated 8 times. She was discharged — but now presents to another ED with acute CP ( C hest P ain ) in association with this current ECG shown in Figure-1. Prolonged thrombectomy effort was unsuccessful. Post PCI angiogram is shown below.
Second , when you have a rhythm problem, you are likely to be able to fix the problem with electricity (cardioversion, defibrillation, pacing). Making a specific ECG Diagnosis (less important in the ED) Without reading the below, I suspected posterior fascicular VT. Again the clinical history is helpful.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content